 E-submission
E-submission
Articles
- Page Path
- HOME > J Mov Disord > Volume 15(2); 2022 > Article
-
Brief communication
Automatic Measurement of Postural Abnormalities With a Pose Estimation Algorithm in Parkinson’s Disease -
Jung Hwan Shin1
 , Kyung Ah Woo1, Chan Young Lee1, Seung Ho Jeon2, Han-Joon Kim1, Beomseok Jeon1
, Kyung Ah Woo1, Chan Young Lee1, Seung Ho Jeon2, Han-Joon Kim1, Beomseok Jeon1 -
Journal of Movement Disorders 2022;15(2):140-145.
DOI: https://doi.org/10.14802/jmd.21129
Published online: January 19, 2022
1Department of Neurology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea
2Department of Neurology, Jeonbuk National University Hospital, Jeonbuk National University College of Medicine, Jeonju, Korea
- Corresponding author: Beomseok Jeon, MD, PhD Department of Neurology, Seoul National University College of Medicine, 101 Daehak-ro, Jongno-gu, Seoul 03080, Korea / Tel: +82-2-2072-2876 / Fax: +82-2-2072-0839 / E-mail: brain@snu.ac.kr
Copyright © 2022 The Korean Movement Disorder Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Objective
- This study aims to develop an automated and objective tool to evaluate postural abnormalities in Parkinson’s disease (PD) patients.
-
Methods
- We applied a deep learning-based pose-estimation algorithm to lateral photos of prospectively enrolled PD patients (n = 28). We automatically measured the anterior flexion angle (AFA) and dropped head angle (DHA), which were validated with conventional manual labeling methods.
-
Results
- The automatically measured DHA and AFA were in excellent agreement with manual labeling methods (intraclass correlation coefficient > 0.95) with mean bias equal to or less than 3 degrees.
-
Conclusion
- The deep learning-based pose-estimation algorithm objectively measured postural abnormalities in PD patients.
- Patients and imaging protocol
- We prospectively enrolled PD patients with camptocormia who visited the movement disorder clinic at Seoul National University Hospital from June to December 2020. The diagnosis of camptocormia was determined by neurological examination by a movement disorder expert (BJ) without a detailed definition of flexed angle. The patients were clinically diagnosed with PD based on the UK Brain Bank criteria [9]. We excluded patients who were unable to stand unassisted or wore clothes that covered the body shape. We included participants who could simply remove the clothes covering the body shape (e.g., an outer jacket) but excluded those in which the clothes could not be easily changed in the outpatient clinic (e.g., long skirt or loosened sweater).
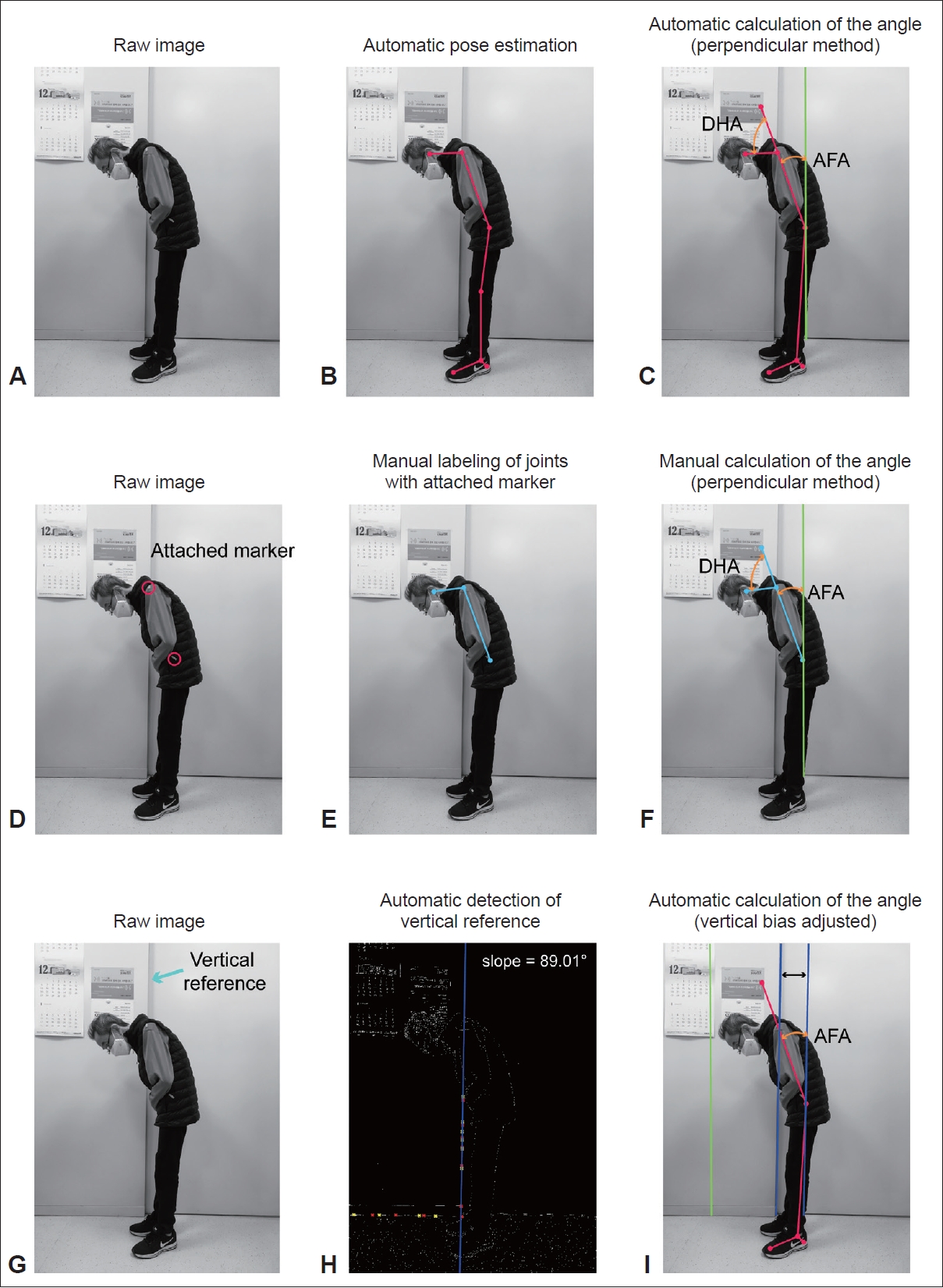
- The patients were asked to stand relaxed in front of a wall at the clinic. We took lateral pictures of the patients with a smartphone camera (iPhone 6s, Apple, Cupertino, CA, USA) The lens was located in a position parallel to the patient’s hip (Figure 1). The vertical reference (vertical line by the door) was used to take pictures as perpendicular to the floor as possible. For validation, we marked the position of the left great trochanter and the left acromion with a detachable sticker (3M, Saint Paul, MN, USA) after manual palpation of the joint (Figure 1D-F). In cases where the patient’s forearm or hand occluded the position of the hip joint, we took an additional picture of the patients as much as possible, with hands cleared from the hip joint while standing in the same posture (Supplementary Figure 1 in the online-only Data Supplement). All participants gave written informed consent, and the institutional review board of Seoul National University Hospital approved this study (1908-175-1059, 2106-099-1228).
- Automatic joint estimation and vertical reference detection
- For the automatic measurements, we used an open-source deep-learning-based position-tracking algorithm (Openpose [8]). The algorithm automatically detects 25 joints (nose and bilateral eye, ear, shoulder, elbow, wrist, hip, knee, ankle, big toe, little toe and heel) without any attached markers. Then, we subtracted the 2D position of the left ear, shoulder, hip and ankle (Figure 1). To detect the angle of the vertical reference (contour of the door) within the frame, the image was transformed to the binary image, and the vertical edge within the image was detected with the Canny method followed by the Hough transform (Figure 1G-I). The vertical line with the longest length was chosen and was validated (JHS) by visual inspection. We calculated the degree of slope and calculated the Anterior flexion angle (AFA) with an adjusted vertical reference (Figure 1I).
- Measurement of postural angles with the pose-estimation method and manual labeling method
- The AFA was defined as the angle between the vertical reference and the lines connecting the hip joint and shoulder joint. The dropped head angle (DHA) was defined as the angle between the lines connecting the hip-acromion and acromion-ear (Figure 1) [5,10]. Additionally, we used the position of the great trochanter, acromion and lateral malleolus of the ankle to calculate the AFA (Supplementary Figure 2 in the online-only Data Supplement) [6].
- The manual measurement of AFA and DHA was performed with CamptoApp [6] (Department of Neurology, UKSH, Kiel University, Kiel, Germany) by a doctor (KAW) who was blinded to any clinical information or automatic measurement of camptocormia. For the manual measurements, the positions of the acromion and great trochanter were marked at the position of the detachable stickers in the photograph (Figure 1).
- Statistical analysis
- The intraclass correlation coefficient (ICC) was used to validate the image-based automatic detection of the camptocormia angle. We used the two-way mixed-effects model with the relationship defined as absolute agreement [11]. All analyses were performed using MATLAB 2020a (Mathworks, Natick, MA, USA).
MATERIALS & METHODS
- Twenty-eight PD patients were prospectively enrolled. Male patients comprised 39.3% (11/28) of the participants. The mean age (standard deviation) of the participants was 59.0 (6.2) years, with a mean disease duration (standard deviation) of 13.9 (7.2) years. The mean levodopa equivalent dose (standard deviation) was 785.96 (373.46).
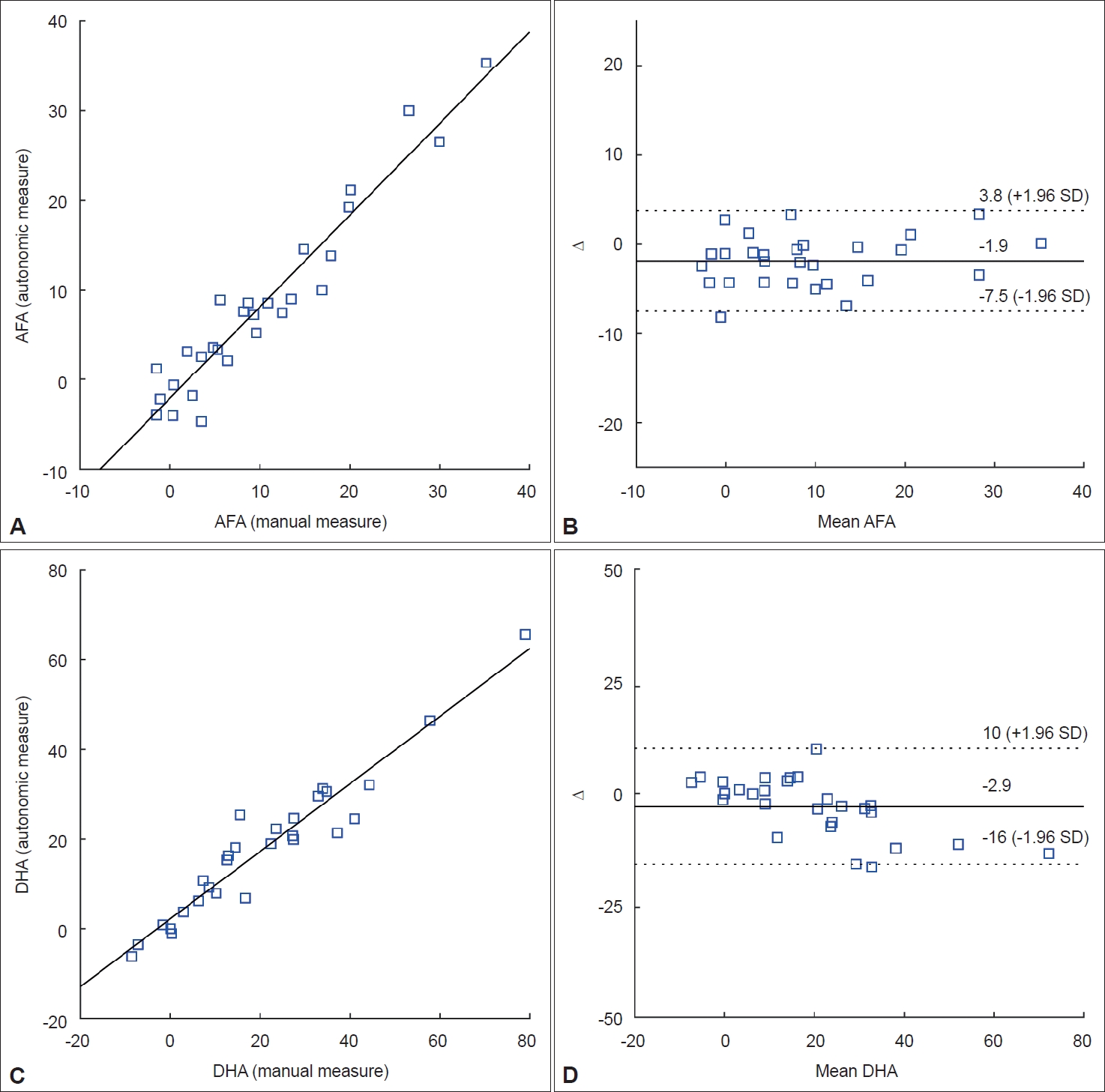
- Examples of automatic and manual measurements of the AFA and DHA are shown in Figure 1A and B, respectively. The mean (standard deviation) anterior AFA and DHA with the manual measurements were 10.57 (9.61) and 21.45 (19.99) degrees, respectively. The ICC [95% confidence interval] was 0.971 [0.889–0.989] and 0.953 [0.895–0.979] with mean (standard deviation) biases of 1.85 (2.87) and 3.00 (6.69) degrees with the AFA and DHA, respectively. Overall, the performance of the algorithm was in excellent agreement with the manual labeling method (ICC > 0.95), and the mean bias was equal to or less than 3 degrees. The bias and standard deviation are also shown with the Bland-Altman plot (Figure 2).
- We automatically detected the vertical reference within the image, calculated the slope and adjusted the AFA (Figure 1G-I). The mean (standard deviation) bias in the vertical reference was 0.91 (1.26) degrees. We also calculated the AFA with the malleolar-hip joint line (Supplementary Figure 2 in the online-only Data Supplement), and the calculated mean AFA (standard deviation) was 8.69 (12.59) degrees.
- In 7 patients whose hip joint was occluded by the forearm, additional photos of the forearm cleared from the hip joint were analyzed (Supplementary Figure 1 in the online-only Data Supplement). We compared the calculated AHA and DHA from two situations (occluded hip joint vs. visible hip joint). The mean (standard deviation) differences in the AHA and DHA were 0.80 (1.94) and 3.59 (5.11) degrees, respectively.
RESULTS
- In this study, we showed that the deep-learning-based pose-estimation algorithm can reliably measure abnormal postural angles in PD patients (ICC > 0.95). The algorithm is fully automated and does not require attached markers. Additionally, the algorithm can adjust the bias of the vertical reference. Thus, the algorithm has the potential to be widely used in research and clinical practice for a reliable measure of abnormal postures in PD. We have developed this algorithm as an application that can be downloaded online (https://github.com/LuckyFace/Posture-analyzer).
- We measured the AFA and DHA using the greater trochanter, acromion and acoustic canal [5,10]. The AFA measured with this method uses a vertical line that may be slightly tilted while taking photos [6]. To solve this issue, we showed that we can measure the AFA with an adjusted vertical axis by the automatic detection of the slope of the vertical reference within the frame (Figure 1G-I). Of note is that the mean vertical bias was approximately 1 degree, which suggests that with an adequate protocol, the vertical bias can be minimal. Additionally, we used the ankle joint to measure the AFA (Supplementary Figure 2 in the online-only Data Supplement) [6]. However, the previous methods using the malleolar method used C7, L5 of the spine and the lateral malleolus and thus did not directly correspond to our methods using the greater trochanter of the femur and the acromion. Measuring the camptocormia angle using the greater trochanter, acromion and lateral malleolus of the ankle has not been validated in PD patients and thus requires further investigation.
- The automatic algorithm could measure the AFA in the case of hip joint occlusion by the forearm. The bias between the two situations (occluded hip joint vs. visible hip joint) was within 5 degrees.
- There are several limitations of the study. First, our study did not enroll age-matched healthy controls or patients without postural abnormalities. Second, we did not consider whether the patients were in medication on and off states when taking photographs. Third, the methods using the lateral malleolus were not validated with the manual labeling method. As the initial design of the study was to validate the automated algorithm using the joint positions of the acoustic canal, acromion and greater trochanter, the lateral malleolus was not visible in most of the participants (24/28). Fourth, our method cannot measure upper camptocormia as previously reported, as the pose-estimation algorithm cannot detect the fulcrum [6]. Two participants among the 28 patients showed abnormal upper truncal flexion based on previously proposed criteria [7]. Furthermore, our algorithm could not calculate camptocormia angles using C7 or L5 [6,7], as the algorithm cannot detect the C7 or L5 position. A future revision of the pose-estimation technique would enable the expansion of the current algorithm. Last, we did not evaluate lateral flexion of the patients [3,12], but as the pose-estimation algorithm labels bilateral shoulders and hip joints, we expect that the algorithm would successfully measure the lateral flexion angle, which should be evaluated in the future.
DISCUSSION
Supplementary Materials
Supplementary Figure 1.
Supplementary Figure 2.
-
Conflicts of Interest
The authors have no financial conflicts of interest.
-
Funding Statement
This research was supported by an investigator award from the Korea Movement Disorder Society (KMDS).
-
Author Contributions
Conceptualization: Jung Hwan Shin, Beomseok Jeon. Data curation: Jung Hwan Shin. Formal analysis: Jung Hwan Shin. Funding acquisition: Jung Hwan Shin. Investigation: Jung Hwan Shin. Methodology: Jung Hwan Shin. Project administration: Jung Hwan Shin. Resources: Jung Hwan Shin. Software: Jung Hwan Shin. Supervision: Jung Hwan Shin, Beomseok Jeon. Validation: Jung Hwan Shin. Visualization: Jung Hwan Shin. Writing—original draft: Jung Hwan Shin. Writing—review & editing: all authors.
Notes
- 1. Doherty KM, van de Warrenburg BP, Peralta MC, Silveira-Moriyama L, Azulay JP, Gershanik OS, et al. Postural deformities in Parkinson’s disease. Lancet Neurol 2011;10:538–549.ArticlePubMed
- 2. Tiple D, Fabbrini G, Colosimo C, Ottaviani D, Camerota F, Defazio G, et al. Camptocormia in Parkinson disease: an epidemiological and clinical study. J Neurol Neurosurg Psychiatry 2009;80:145–148.ArticlePubMed
- 3. Tinazzi M, Fasano A, Geroin C, Morgante F, Ceravolo R, Rossi S, et al. Pisa syndrome in Parkinson disease: an observational multicenter Italian study. Neurology 2015;85:1769–1779.ArticlePubMed
- 4. Kashihara K, Ohno M, Tomita S. Dropped head syndrome in Parkinson’s disease. Mov Disord 2006;21:1213–1216.ArticlePubMed
- 5. Ando Y, Fujimoto KI, Ikeda K, Utsumi H, Okuma Y, Oka H, et al. Postural abnormality in Parkinson’s disease: a large comparative study with general population. Mov Disord Clin Pract 2019;6:213–221.ArticlePubMedPMC
- 6. Margraf NG, Wolke R, Granert O, Berardelli A, Bloem BR, Djaldetti R, et al. Consensus for the measurement of the camptocormia angle in the standing patient. Parkinsonism Relat Disord 2018;52:1–5.ArticlePubMed
- 7. Fasano A, Geroin C, Berardelli A, Bloem BR, Espay AJ, Hallett M, et al. Diagnostic criteria for camptocormia in Parkinson’s disease: a consensus-based proposal. Parkinsonism Relat Disord 2018;53:53–57.ArticlePubMedPMC
- 8. Cao Z, Hidalgo G, Simon T, Wei SE, Sheikh Y. OpenPose: realtime multiperson 2D pose estimation using part affinity fields. IEEE Trans Pattern Anal Mach Intell 2021;43:172–186.ArticlePubMed
- 9. Hughes AJ, Daniel SE, Kilford L, Lees AJ. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: a clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiatry 1992;55:181–184.ArticlePubMedPMC
- 10. Kashihara K, Imamura T. Clinical correlates of anterior and lateral flexion of the thoracolumbar spine and dropped head in patients with Parkinson’s disease. Parkinsonism Relat Disord 2012;18:290–293.ArticlePubMed
- 11. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med 2016;15:155–163.ArticlePubMedPMC
- 12. Baik JS, Kim JY, Park JH, Han SW, Park JH, Lee MS. Scoliosis in patients with Parkinson’s disease. J Clin Neurol 2009;5:91–94.ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
- Three‐Dimensional Mesh Recovery from Common 2‐Dimensional Pictures for Automated Assessment of Body Posture in Camptocormia
Robin Wolke, Olga Gavriliuc, Oliver Granert, Günther Deuschl, Nils G. Margraf
Movement Disorders Clinical Practice.2023; 10(3): 472. CrossRef - Assessment of Axial Postural Abnormalities in Parkinsonism: Automatic Picture Analysis Software
Carlo Alberto Artusi, Christian Geroin, Gabriele Imbalzano, Serena Camozzi, Stefano Aldegheri, Leonardo Lopiano, Michele Tinazzi, Nicola Bombieri
Movement Disorders Clinical Practice.2023; 10(4): 636. CrossRef - Camera- and Viewpoint-Agnostic Evaluation of Axial Postural Abnormalities in People with Parkinson’s Disease through Augmented Human Pose Estimation
Stefano Aldegheri, Carlo Alberto Artusi, Serena Camozzi, Roberto Di Marco, Christian Geroin, Gabriele Imbalzano, Leonardo Lopiano, Michele Tinazzi, Nicola Bombieri
Sensors.2023; 23(6): 3193. CrossRef
Comments on this article
 PubReader
PubReader ePub Link
ePub Link Cite
Cite

