 E-submission
E-submission
Articles
- Page Path
- HOME > J Mov Disord > Volume 12(1); 2019 > Article
-
Letter to the editor
Novel Ferritin Light Chain Gene Mutation in a Korean Patient with Neuroferritinopathy -
So Hoon Yoon1, Nan Young Kim2,3, Yun Joong Kim2,3, Chul Hyoung Lyoo1

-
Journal of Movement Disorders 2019;12(1):63-65.
DOI: https://doi.org/10.14802/jmd.18062
Published online: January 30, 2019
1Department of Neurology, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea
2Hallym Institute of Translational Genomics & Bioinformatics, Hallym University Medical Center, Anyang, Korea
3Ilsong Institute of Life Science and Department of Neurology, Hallym University, Anyang, Korea
- Corresponding author: Chul Hyoung Lyoo, MD, PhD, https://orcid.org/0000-0003-2231-672X Department of Neurology, Gangnam Severance Hospital, Yonsei University College of Medicine, 20 Eonju-ro 63-gil, Gangnam-gu, Seoul 06229, Korea / Tel: +82-2-2019-3326 / Fax: +82-2-3462-5904 / E-mail: lyoochel@yuhs.ac
• Received: November 23, 2018 • Revised: December 8, 2018 • Accepted: December 20, 2018
Copyright © 2019 The Korean Movement Disorder Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- This study was financially supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIP) (No. 2015R1C1A2A01054507) and the Basic Science Research Program through the NRF funded by the Ministry of Science, ICT & Future Planning (2017R1A2B2006694). This study was approved by the institutional review board of Gangnam Severance Hospital.
Acknowledgments
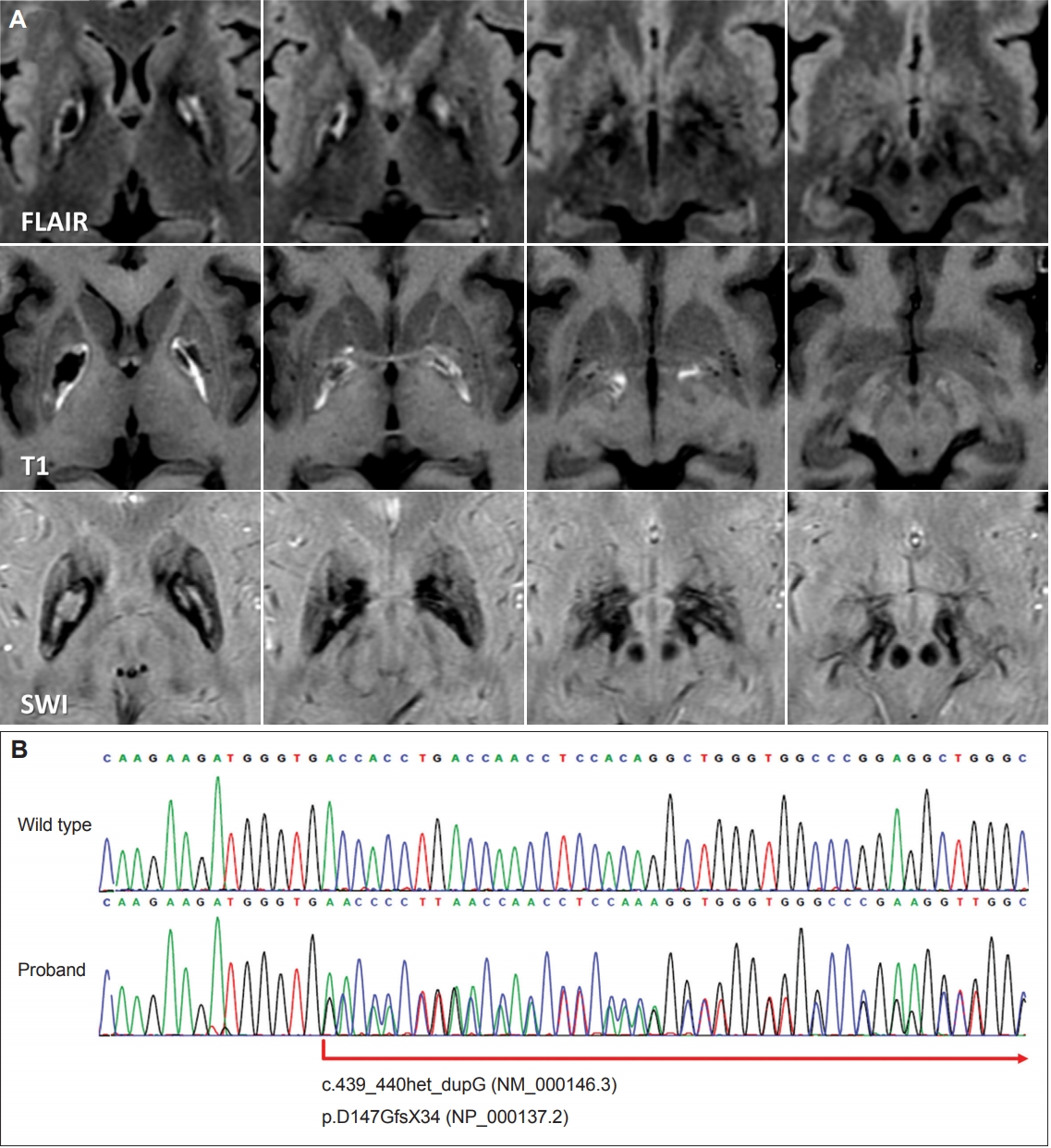
Figure 1.Brain MR images and the DNA sequence of the neuroferritinopathy patient. A: Fluid-attenuated inversion recovery (FLAIR) MR images show a trilamellar cystic lesion in the pallidum. T1-weighted and susceptibility-weighted (SWI) MR images show a cystic core and a surrounding rim of iron deposition. B: Sanger sequencing results of the proband showing a novel frameshift mutation (c.439_440het_dupG, NM_000146.3) in the FTL1 gene.
- 1. Chinnery PF, Crompton DE, Birchall D, Jackson MJ, Coulthard A, Lombes A, et al. Clinical features and natural history of neuroferritinopathy caused by the FTL1 460InsA mutation. Brain 2007;130:110–119.ArticlePubMedPDF
- 2. Ohta E, Nagasaka T, Shindo K, Toma S, Nagasaka K, Ohta K, et al. Neuroferritinopathy in a Japanese family with a duplication in the ferritin light chain gene. Neurology 2008;70:1493–1494.ArticlePubMed
- 3. Kubota A, Hida A, Ichikawa Y, Momose Y, Goto J, Igeta Y, et al. A novel ferritin light chain gene mutation in a Japanese family with neuroferritinopathy: description of clinical features and implications for genotypephenotype correlations. Mov Disord 2009;24:441–445.ArticlePubMed
- 4. Nishida K, Garringer HJ, Futamura N, Funakawa I, Jinnai K, Vidal R, et al. A novel ferritin light chain mutation in neuroferritinopathy with an atypical presentation. J Neurol Sci 2014;342:173–177.ArticlePubMedPMC
- 5. Ni W, Li HF, Zheng YC, Wu ZY. FTL mutation in a Chinese pedigree with neuroferritinopathy. Neurol Genet 2016;2:e74.ArticlePubMedPMC
- 6. Levi S, Rovida E. Neuroferritinopathy: from ferritin structure modification to pathogenetic mechanism. Neurobiol Dis 2015;81:134–143.ArticlePubMedPMC
- 7. Batla A, Adams ME, Erro R, Ganos C, Balint B, Mencacci NE, et al. Cortical pencil lining in neuroferritinopathy: a diagnostic clue. Neurology 2015;84:1816–1818.ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
Citations to this article as recorded by 
- Transcriptome Profile in the Mouse Brain of Hepatic Encephalopathy and Alzheimer’s Disease
Young-Kook Kim, Yoon Seok Jung, Juhyun Song
International Journal of Molecular Sciences.2022; 24(1): 675. CrossRef - Pathogenic mechanism and modeling of neuroferritinopathy
Anna Cozzi, Paolo Santambrogio, Maddalena Ripamonti, Ermanna Rovida, Sonia Levi
Cellular and Molecular Life Sciences.2021; 78(7): 3355. CrossRef - A Patient with Neuroferritinopathy Presenting with Juvenile-Onset Voice Tremor
Chan Wook Park, Nan Young Kim, Yun Joong Kim, Sook Keun Song, Chul Hyoung Lyoo
Journal of Movement Disorders.2020; 13(1): 66. CrossRef - Brain MRI Pattern Recognition in Neurodegeneration With Brain Iron Accumulation
Jae-Hyeok Lee, Ji Young Yun, Allison Gregory, Penelope Hogarth, Susan J. Hayflick
Frontiers in Neurology.2020;[Epub] CrossRef - Iron, Ferritin, Hereditary Ferritinopathy, and Neurodegeneration
Barry B. Muhoberac, Ruben Vidal
Frontiers in Neuroscience.2019;[Epub] CrossRef
Comments on this article
 PubReader
PubReader ePub Link
ePub Link Cite
Cite
