123I-Metaiodobenzylguanidine Myocardial Scintigraphy in Lewy Body-Related Disorders: A Literature Review
Article information
Abstract
Lewy body-related disorders are characterized by the presence of Lewy bodies and Lewy neurites, which have abnormal aggregations of α-synuclein in the nigral and extranigral areas, including in the heart. 123I-metaiodobenzylguanidine (MIBG) scintigraphy is a well-known tool to evaluate cardiac sympathetic denervation in the Lewy body-related disorders. MIBG scintigraphy showed low uptake of MIBG in the Lewy body-related disorders, including Parkinson’s disease, dementia with Lewy bodies, pure autonomic failure and rapid eye movement sleep behavior disorder. This review summarizes previous results on the diagnostic applications of MIBG scintigraphy in Lewy body-related disorders.
INTRODUCTION
Since 123I-metaiodobenzylguanidine (MIBG) scintigraphy was approved by the Health and Welfare Ministry of Japan in 1992 [1], MIBG has typically been used to study the regional denervation of the heart in ischemic heart diseases, such as acute coronary syndromes and cardiomyopathies [2-5]. In the mid- 1990s, clinical trials of MIBG began in the field of neurology [6-12], and many countries have since begun to use MIBG scintigraphy to study related movement disorders and dementia [1].
MIBG scintigraphy is a diagnostic technique that is used to detect and evaluate sympathetic denervation [13]. In the last few years, MIBG scintigraphy has been reported as a useful tool for diagnosing Parkinson’s disease (PD) [9] and differentiating PD from other parkinsonisms, such as multiple system atrophy (MSA) [12], progressive supranuclear palsy (PSP) [8], vascular parkinsonism and drug-induced parkinsonism [14,15], and even from essential tremor [16]. Recently, MIBG scintigraphy has been used to discriminate dementia with Lewy bodies (DLB) from Alzheimer’s disease (AD) [17] and to predict the conversion to probable DLB [18]. Therefore, it is necessary to organize the scattered comprehensive MIBG studies on neurodegenerative disorders. The first purpose of this study is to systematically review the diagnostic application of MIBG scintigraphy in neurodegenerative disorders. Additionally, we investigate the potential usefulness of MIBG scintigraphy for the early detection, prognostic prediction and differentiation of various neurodegenerative disorders.
Neuroanatomy of sympathetic innervation
Sympathetic innervation of the heart originates in the intermediolateral column of the thoracic spinal cord, segments 1 to 5 [19]. The first synapses form in the upper-most thoracic and cervical ganglia [19]. Postganglionic noradrenergic sympathetic fibers accompany the blood vessels to the heart and enter into the myocardium [20,21].
Fundamentals of MIBG scintigraphy
MIBG is a pharmacologically inactive urea derivative that, like noradrenaline, is taken up by adrenergic cells via the human norepinephrine transporter mechanism, stored in vesicles, and secreted in response to a variety of stimuli [19,22-25]. Guanethidine may be chemically modified to MIBG [26-28]. MIBG can be labeled with radioactive iodine (most commonly 123Iodine) to become 123I-MIBG, and it is taken up by the postganglionic, presynaptic nerve endings [1,5,26-28]. Radiolabeled MIBG is considered an established sympathetic neuron imaging agent that is useful to study organs that are richly innervated by the sympathetic nervous system [1,5,27,28]. After depolarization, MIBG is released into the synaptic cleft, similar to norepinephrine, but it is not metabolized [1,5,27,28]. 123I-MIBG uptake has been shown to correlate with adrenergic innervation [1,5,27]. Therefore, 123I-MIBG scintigraphy reveals not only the presence of noradrenergic innervation but also its functional capability [19].
The MIBG scintigraphy method and semiquantitative measurements
Before the examination, it is necessary to establish an appropriate withdrawal period for interfering drugs, taking into account their biological half-lives [5]. For the scintigraphic method of myocardial innervation imaging, 123I-MIBG is intravenously administered at rest, and early (from 10 to 30 min after injection) and delayed (from 3 to 4 h after injection) images are obtained [5,21,26]. Planar images with an anterior view are adequate for the evaluation of cardiac sympathetic function [29]. Tomographic images [single photon emission computed tomography (SPECT)] are often acquired to evaluate the three-dimensional myocardial uptake pattern [1,5,29,30].
Cardiac MIBG uptake in the early phase primarily reflects the integrity and distribution of the presynaptic sympathetic system and the density of the presynaptic cardiac sympathetic nerve endings, whereas the delayed imaging phase also reflects the presynaptic functional tone of the cardiac sympathetic nerve [21,26]. During the hours that follow, MIBG actively enters the sympathetic nerve terminals, mainly in the left ventricular wall, and is quickly washed out in non-neuronal tissue. The delayed phase measurement at 3 to 4 hours after radiotracer injection reflects the active neuronal uptake of MIBG without passive transfer and is recommended for diagnostic studies [21,31,32].
The most common semi-quantitative indices used to interpret the myocardial innervation images are the heart to mediastinum ratio (H/M) and the washout rate obtained from the anterior planar images [28]. Regions of interest (ROIs) are set in the heart (H; target region) and the mediastinum (M; background region) in the early and delayed images to obtain the mean count in each ROI, after which the H/M ratio is calculated [28]. The degree of MIBG accumulation in the heart is evaluated by the H/M ratio. The washout rate is an index that indicates the rate at which MIBG is washed out between the early image and the delayed image by comparing the cardiac counts in the two images [28]. The normal values of these indices have been calculated by performing MIBG scintigraphy in control patients and can differ between various institutions depending on acquisition conditions [1,5,19,28-30]. The normal limit is based on the computation of the 95th percentile of the results in the control group [28].
Most current anti-Parkinson drugs, except MAOB inhibitors, do not affect MIBG uptake [8,10,31,33], but several substances can interfere with MIBG uptake [19,31]. MAO-B inhibitors reduce the H/M ratios of MIBG, and other drugs, such as sympathomimetic agents (e.g., L-threo-DOPS), tricyclic and tetracyclic antidepressants, serotonin reuptake inhibitors, calcium antagonists, and cardiac glycosides, competitively inhibit MIBG uptake into the sympathetic nerve terminals [19]. Therefore, these drugs should be avoided prior to cardiac sympathetic nervous system assessment, and the results need to be carefully interpreted when patients taking these drugs are analyzed by MIBG scintigraphy (Table 1).
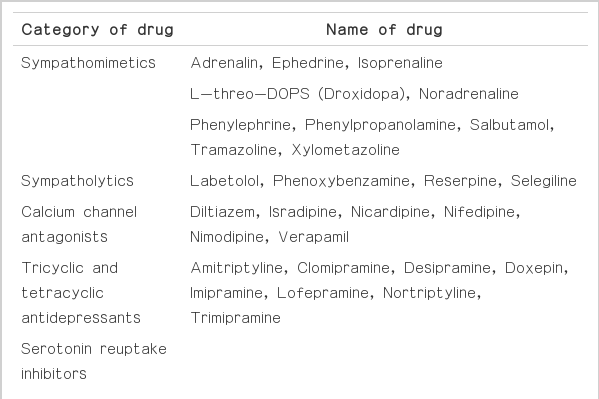
List of drugs that interfere with MIBG uptake
Although cardiac MIBG scintigraphy is a popular diagnostic tool in PD, MIBG scintigraphy has also been evaluated in other organs associated with the sympathetic nervous system, such as the lungs, parotid gland, thyroid, liver and muscle tissues [34-36]. Abnormalities in MIBG uptake are reportedly rare in these organs, although one study [34,36] suggested that thyroid MIBG uptake was reduced in PD [35].
Application of MIBG scintigraphy in various neurological disorders
MIBG scintigraphy was originally developed to assess postganglionic presynaptic cardiac sympathetic nerve endings in a variety of cardiac diseases, including congestive heart failure, ischemic heart disease, coronary artery disease, vasospastic angina pectoris and cardiomyopathy [34,37]. Patients with autonomic failure associated with various neurological diseases of the central and peripheral nervous system showed a reduction of myocardial uptake in MIBG scintigraphy, suggesting cardiac sympathetic dysfunction or denervation [6,34,38-40].
PARKINSON’S DISEASE AND PARKINSON PLUS SYNDROMES
Lewy bodies are intra-cytoplasmic eosinophilic inclusions with a hyaline core and a pale halo that is mainly composed of aggregated α-synuclein [19,41]. The sympathetic nervous system is regularly affected in Lewy body-related disorders [42]. PD is the most common neurodegenerative disorder displaying Lewy body pathology in the brain [43].
Although differential diagnosis of PD from other parkinsonisms is difficult because of the clinical overlap of parkinsonian symptoms [37], the clinical differentiation is very important for deciding upon drug therapy, monitoring patient response to therapy and determining patient prognosis [26].
Parkinson’s disease
Because postganglionic sympathetic failure in PD had been reported [44], MIBG uptake is reportedly decreased in nearly all patients with PD [7-12,45,46], regardless of orthostatic hypotension [10,12,45,46]. The MIBG uptake is reduced even in patients with very early PD as determined using the Hoehn & Yahr (H&Y) staging system, who do not manifest clinically significant signs or symptoms of autonomic dysfunction [8,10,47,48]; reduced MIBG uptake could indicate the eventual disease severity [48,49]. These findings suggest that MIBG scintigraphy could be a useful tool for detecting PD [27,48]. A study showed that the H/M ratios in both the early and delayed images had a tendency to decrease with the progression of the H&Y stages, although this correlation was not statistically significant [48,50].
MIBG scintigraphy also showed a relationship between MIBG uptake and PD phenotype [49]. Generally, MIBG uptake or the H/M ratio is inversely correlated with bradykinesia, rigidity and axial symptoms such as speech, posture and gait [51-53]. However, a study on the predictive value of MIBG scintigraphy regarding the severity and progression of the Parkinsonian motor symptoms suggested that MIBG scintigraphy predicts the velocity of progression on the rigidity and axial symptoms, but not the other motor symptoms of resting tremor, postural tremor and bradykinesia [54].
PD patients could show many non-motor symptoms before the occurrence of motor symptoms. PD cases that initially present these non-motor symptoms are referred to as pre-motor PD, and these cases can also show low MIBG uptake, which suggests that this a good measurement to detect preclinical-stage PD [55]. Olfactory dysfunction, including hyposmia and anosmia, is an important non-motor symptom in PD [56]. Although there have been no large correlation studies between olfactory dysfunction and MIBG scintigraphy, an asymptomatic carrier of an α-synuclein gene mutation showed severe sympathetic myocardial denervation but a normal olfactory test [57]. This report suggests that cardiac sympathetic neuronal degeneration precedes dopaminergic nerve dysfunction [57].
Scans without evidence of dopaminergic defects (SWEDDs) are defined as cases with normal dopamine transporter scans performed in the clinical diagnosis of PD [58,59], and SWEDD cases can be challenging to diagnose and are often misdiagnosed as PD. A recent study also showed that MIBG scintigraphy may help to differentiate patients with SWEDDs from patients with PD [60]. The H/M ratios and washout rate in the MIBG scintigraphy of the SWEDDs group differed from those of both the control and PD groups [60].
Studies of MIBG uptake in genetic PD showed inconsistent results [57,61-64]. Some patients with genetic mutations (in parkin or PARK2, DJ-1, PINK1, and leucine-rich repeat kinase 2) showed normal cardiac MIBG uptake, but others showed lower MIBG uptake [61-64]. Asymptomatic carriers with α-synuclein gene mutations showed low MIBG uptake and tended to develop Lewy body disorders later [57,65].
Differential diagnosis of PD from Parkinson plus syndromes (Table 2)
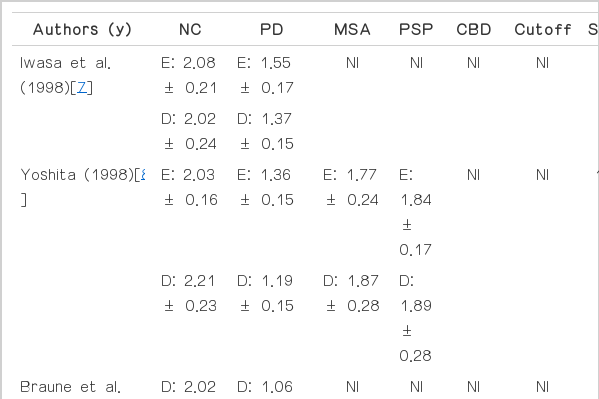
Comparison of the heart to mediastinum ratio in Parkinson’s disease and other parkinsonism disorders
The sensitivity and specificity of MIBG scintigraphy in differential diagnosis between PD and other parkinsonism disorders ranged from 71 to 100% and from 50 to 100%, respectively, with pooled estimates of 88% [95% confidence interval (CI) 86–90%] and 85% (95% CI 81–88%) [8-10,15,16,27,34,36,48,50,66-75]. In terms of diagnostic performance, many studies have indicated that MIBG scintigraphy is usually a sensitive, but not specific, test for PD [8,15,48,67,68,73].
Autonomic failure is representative of several non-motor deficits that are often encountered in PD [55,68,76-78]. Autonomic failure in PD includes gastrointestinal, sudomotor, thermoregulation, and bladder abnormalities [79-81] and may manifest as urinary frequency/urgency or incontinence, chronic constipation, drooling, erectile failure in men, abnormal sweating, or orthostatic intolerance [81-83]. MSA is a representative neurodegenerative disorder that is characterized by a combination of parkinsonism and autonomic failure [84]. Although autonomic failure is more severe in MSA than in PD 80,85], it also occurs in PD [77,78]. Orthostatic hypotension is a common feature in PD that results from sympathetic post-ganglionic noradrenergic denervation [19,26,44,86-88]. Systematic investigations using MIBG scintigraphy showed a reduced MIBG uptake in PD compared with MSA [7,8,10-12,34,36,46,48,49,71,73-75,89-91]. The pooled sensitivity and specificity for differentiating PD and MSA were 90.2% (95% CI: 84.4%, 93.9%) and 81.9% (95% CI: 56.1%, 94.1%), respectively [8,34,36,48,66,67,73,75,91,92]. For differentiating PD and PSP, the pooled sensitivity and specificity were 91.4% (95% CI: 80.5%, 96.5%) and 78.0% (95% CI: 6.8%, 99.4%), respectively [8,10,34,73,74,92].
A few studies reported reduced MIBG uptake in MSA and PSP, although the reductions were smaller than those in PD [48,93,94]. These findings are supported by the evidence that postganglionic impairment also occurs in patients with MSA [95].
Although there are no data on the pooled analysis for differentiating PD and cortico-basal degeneration (CBD), two studies on CBD showed high sensitivity and low specificity of MIBG scintigraphy [34,67]. A comparative study between PD and CBD showed that the early and delayed H/M ratios in the patients with CBD were significantly higher than those in the patients with PD [96].
Both the early and delayed images for the differential diagnosis between PD and Parkinson plus syndromes showed high specificity of MIBG scintigraphy in cases of PD overall and high sensitivity in the advanced stage of PD [48,50]. However, MIBG scintigraphy in early cases showed low sensitivity in the diagnosis of PD [50], despite the gross reduction of MIBG uptake in the early stage of the disease [31].
There have been several studies about the correlation between the functional images of dopaminergic system and that of cardiac sympathetic system. One study showed a good correlation between MIBG uptake and dopamine uptake [97], but another study found no correlation between the two indices [50,94]. Therefore, one study suggested that MIBG scintigraphy is a useful, complementary tool when it is used with dopaminergic neuroimaging [50].
DLB AND DIFFERENTIAL DIAGNOSIS OF DLB FROM AD (Table 3)
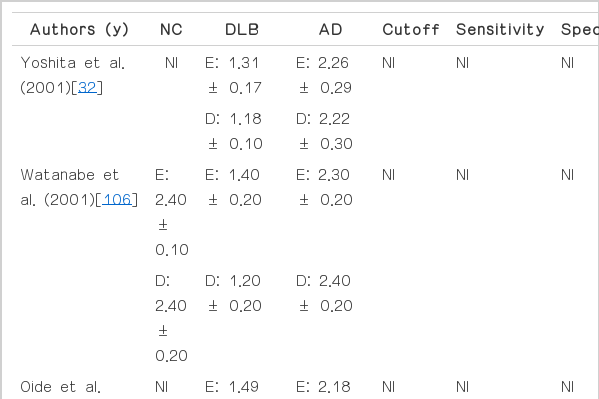
Comparison of the heart to mediastinum ratio in DLB and AD
DLB is a typical disorder with Lewy body pathology [18,19], and cardiac uptake of MIBG is also reduced in patients with DLB [8-12,34,90]. Some studies showed that the H/M ratio of DLB was significantly lower than that of PD [48,98]. MIBG scintigraphy is also a good predictor of the future conversion of possible DLB to probable DLB [18].
DLB is clinically characterized by progressive cognitive decline with fluctuations in cognition and alertness, recurrent visual hallucinations, and parkinsonism [99]. The subgroup with the presence of parkinsonism, visual hallucinations and neuroleptic hypersensitivity had a tendency to have low MIBG uptake, in contrast to fluctuations in cognition and alertness [100]. Although the subgroup with the most severe cognitive impairments showed lower MIBG uptake than those with mild and moderate cognitive impairment, this correlation was not found between 2 groups with mild and moderate cognitive deficits [100]. In this study, the subgroup with orthostatic hypotension showed significantly decreased MIBG uptake only when compared to those without orthostatic hypotension [100].
Because DLB shares clinical and pathological features with AD [101], differential diagnosis between DLB and AD is difficult [102]. Several studies have found no correlation of MIBG scintigraphy with the severity or duration of DLB or AD [32,103-105], but many studies have demonstrated reduced MIBG uptake in DLB compared with AD [32,103,104,106-110]. As with the confirmation of the utility of MIBG scintigraphy in discriminating Lewy body-related disorders from non-Lewy body-related disorders [111], the low H/M ratio of MIBG scintigraphy is a possible diagnostic biomarker for DLB and could give a differential diagnostic value in cases where there is doubt about the diagnosis between DLB and AD [17,108]. Compared to occipital hypoperfusion on SPECT, MIBG scintigraphy is powerful tool in detecting DLB [108,112]. Additionally, MIBG scintigraphy has been reported to be more sensitive than cerebrospinal fluid p-tau in terms of differentiating between DLB and AD [109]. In contrast to several studies that reported a normal H/M ratio [32,106], one study found that AD also could show a low H/M ratio, similar to that of PD [48]. This result suggests a relationship between Lewy body pathology and cardiac sympathetic neuronal degeneration in AD [48], whereas the other study found no evidence of significantly low MIBG uptake in AD patients with extrapyramidal sign [104,113].
In terms of diagnostic performance, the pooled sensitivity of MIBG scintigraphy for the detection of DLB was 98%, and the pooled specificity for the differential diagnosis of DLB from other dementias was 94% [99].
However, a lack of pathological data in the discrimination of DLB from AD is also a limitation of MIBG scintigraphy; AD pathology and Lewy body pathology frequently coexist in DLB and AD.
Rapid eye movement sleep behavior disorder
Rapid eye movement sleep behavior disorder (RBD) is found in various neurodegenerative disorders known as synucleinopathies, including PD, DLB and MSA [114], and tauopathies, like AD, PSP and CBD [115]. Patients with synucleinopathies are more likely to have RBD and tend to show RBD in the early stages of the disease compared to those with non-synucleinopathies [114,116-118].
Patients with RBD have Lewy body pathology, which is a common denominator of Lewy body-related disorders such as PD and DLB [119]. Although the prevalence of RBD in the elderly (people of age 70 years or above) was 0.38% [120], PD developed in 38% of those patients within 3.7 years [115,121]. Since the mid-2000s, low MIBG uptake has been reported in patients with RBD [63,111-113]. The low MIBG uptake in RBD patients was similar to those with PD and DLB, or more reduced than in those with early-stage PD [71,122-125]. In addition, a recent study suggests that cardiac denervation precedes nigrostriatal damage in RBD patients [126]. These findings support the hypothesis that RBD is a risk factor for future PD development and could be a marker for predicting PD [121,127,128]. Therefore, RBD patients should be regularly followed up by clinicians because they are good candidates to test the effects of neuroprotective agents before parkinsonian symptoms develop [128].
Pure autonomic failure
Pure autonomic failure (PAF) is a synucleinopathy that is based on Lewy body pathology, similar to PD and DLB, but its clinical presentation is similar to that of MSA [115,129]. PAF shows limited dysfunction of the autonomic system, whereas cerebellar ataxia and parkinsonism with autonomic dysfunction also occur in MSA [130,131]. Low MIBG uptake is also observed in PAF, suggesting cardiac sympathetic denervation in PAF [6,74,132]. Therefore, MIBG scintigraphy can differentiate PAF from MSA.
CONCLUSIONS
In conclusion, MIBG scintigraphy is a useful tool not only for differentiating PD from other neurodegenerative disorders with parkinsonism, but also for assessing disease severity and PD phenotypes. MIBG scintigraphy is also a useful tool in the early diagnosis of patients with pre-motor PD. Low MIBG uptake in patients with DLB, similar to patients with PD, can differentiate DLB from other dementias, including AD. RBD is even a predictor of the progression to neurodegenerative disorders such as PD and DLB, and patients with RBD also show low MIBG uptake.
Notes
Conflicts of Interest
The authors have no financial conflicts of interest.
Acknowledgements
We acknowledge the contributions of Yun Joong Kim of the Hallym Institute of Translational Genomics & Bioinformatics, Hallym University Medical Center.