Sleepiness and Depression in Parkinson’s Disease Patients Treated with Ropinirole and Levodopa
Article information
Abstract
Objective
We aimed to investigate the effect of ropinirole on excessive daytime sleepiness (EDS) and depression in Parkinson’s disease (PD) with a large population.
Methods
We conducted a cross-sectional observational study at nine hospitals in Korea between April 24, 2013, and April 22, 2015. We analyzed the demographic and clinical features, other medical history, history of antiparkinsonian medication within 6 months, Hoehn and Yahr stage (HY stage), Unified Parkinson’s Disease Rating Scale (UPDRS) part II and III, Epworth Sleepiness Scale (ESS), and 30-item Geriatric Depression Scale (GDS-30).
Results
Four-hundred-thirteen patients with PD (mean age: 65.2 ± 9.0 years; men: 227 patients) were analyzed. Multivariate logistic regression analysis showed that age at examination, UPDRS II, and GDS-30 were independent risk factors for EDS and that sex, UPDRS II, and ESS were independent risk factors for depression.
Conclusion
Our large group study did not find any significant associations of ropinirole with EDS and depression in Korean PD patients.
Excessive daytime sleepiness (EDS) and depression are common in Parkinson’s disease (PD) patients [1,2]. EDS was reported in 20–50% of PD patients [1]. However, the characteristics of EDS in PD are unclear. The risk factors for EDS are male gender, long disease duration, extent of motor symptoms severity, and dopamine agonist (DA) use [3]. The effect of dopaminergic medication seems to be inconsistent. Generally, EDS appears to be correlated with higher doses of levodopa equivalents [1], but another study showed that EDS is related to low doses of levodopa and high doses of DA [4,5]. Ropinirole, a DA, has also been suggested to be associated with EDS [6], but there are conflicting results [7-11].
Clinically significant depressive symptoms have been reported in 35% of PD patients [2]. Depression is common and even precedes the onset of motor manifestation by many years [12]. The serotonergic and/or noradrenergic system is known to be important in the pathogenesis of depression. In addition, the dopaminergic system may also play a role in the development of depression in PD [12]. Depression is improved by dopaminergic medication, and depressive symptoms appear as medication wears off [12]. It has been reported that ropinirole improves depressive symptoms [8,10], but there is still not enough evidence to support these findings.
Therefore, the aim of this study was to evaluate the effect of ropinirole on EDS and depression in PD patients. We also analyzed the effect of ropinirole on EDS through stratification of dopaminergic medication.
MATERIALS & METHODS
Study design
This was a cross-sectional observational study conducted at nine hospitals in Korea between April 24, 2013, and April 22, 2015. Participants were evaluated during one visit. We collected their demographic and clinical features, other medical history, history of antiparkinsonian medication within 6 months, Hoehn and Yahr stage (HY stage), and scores on the Unified Parkinson’s Disease Rating Scale (UPDRS) part II and III, Epworth Sleepiness Scale (ESS), and 30-item Geriatric Depression Scale (GDS-30). Patients with an ESS score > 10 were classified as having EDS. Patients with GDS-30 > 17 were classified as having depression. Levodopa equivalent daily doses (LEDD) were calculated according to the usual formula [13].
Patients
The inclusion criteria were 1) diagnosis of idiopathic PD as defined by the UK Parkinson’s Disease Society Brain Bank Criteria [14]; 2) patients who had taken antiparkinsonian medications, including ropinirole and levodopa, for more than six months at the time of enrollment; and 3) no changes of the doses of ropinirole and levodopa for more than one month at the time of enrollment. The exclusion criteria were 1) Alzheimer’s dementia and Vascular dementia, clinically diagnosed using the Diagnostic and Statistical Manual of Mental Disorders diagnostic criteria; 2) patients who participated in other clinical trials at the time of enrollment; 3) chronic use of a sedative; 4) history of alcohol abuse; 5) severe comorbid disorders that can affect sleep (i.e., chronic obstructive pulmonary disease, ischemic heart disease, stroke, and painful joint disease, etc.); and 6) having taken pramipexole or other DAs (rotigotine, bromocriptine) within six months of the time of enrollment.
Standard protocol approvals, registrations, and patient consents
The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice Guidelines. This study protocol was approved by the Institutional Review Board of all nine centers (IRB No. 2013-007). All participants provided written, informed consent prior to enrollment.
Statistical analysis
Data are expressed as the means ± standard deviation. Measurements were compared between patients with EDS and without EDS. Measurements were compared between patients with depression and without depression. For univariate analysis, we used the independent t-test and chi-square test. Multivariate logistic regression with the use of backward elimination was performed on variables that were associated with p < 0.20 according to univariate logistic regression. We chose p = 0.20 as the threshold of significance in multivariate analysis as suggested elsewhere as an appropriate threshold [15]. Because the ranges of the total LEDD were very wide, we thought that it might be a bias for the comparison. Therefore, we classified patients into three groups according to the total LEDD, less than the 32nd percentile; 33rd to 66th percentile; and greater that the 67th percentile, and compared the dosage of ropinirole between patients without and with EDS in each group. All statistical analyses were performed using SAS Proprietary Software 9.4 (SAS Institute, Inc., Cary, NC, USA). Values of p < 0.05 were regarded as significant.
RESULTS
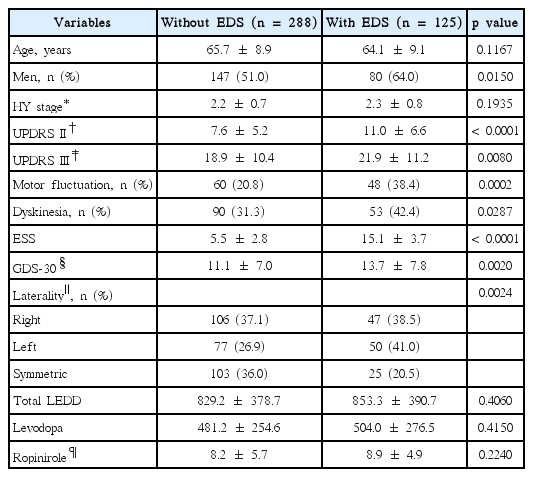
Four-hundred-thirteen of 426 patients who provided informed consent were enrolled. Thirteen patients were excluded; 12 patients did not meet the inclusion criteria, and the other patient’s ESS was missing. The demographic and clinical features are summarized in Table 1.

Demographics and clinical features of 413 patients with Parkinson’s disease
Comparison between patients without and with EDS
Patients with EDS were more likely to be men, had higher UPDRS II & III scores, have more frequent motor fluctuation and dyskinesia, and have more severe depression. There was a significant difference in the laterality of motor symptoms at the time of evaluation. In patients with EDS, the larger proportion of lateralized motor symptoms occurred on the left side. There was no significant difference of the total LEDD between patients without EDS and with EDS. Moreover, there was no significant difference of the levodopa and ropinirole doses (Table 2).
Comparison of Parkinson’s disease patients without and with EDS
Multivariate logistic regression analysis revealed that age at examination, UPDRS II, and depression were independent risk factors for EDS. Total LEDD, levodopa and ropinirole doses were not associated with EDS (Table 3).
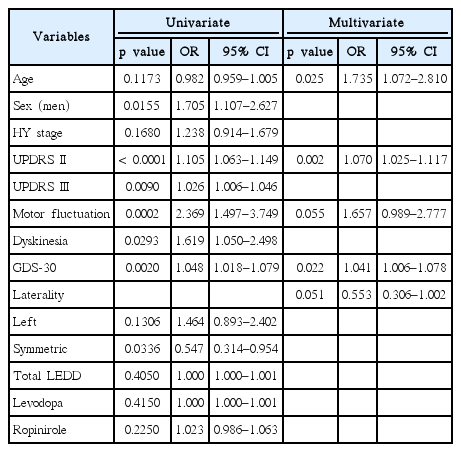
Excessive daytime sleepiness; univariate and multivariate logistic regression analyses
Comparison between patients without and with depression
Patients with depression were more likely to be women; had a higher HY stage as well as UPDRS II and UPDRS III scores; had more severe ESS; and had a higher GDS-30 score. Total LEDD, levodopa dose, and ropinirole dose were not different between patients without and with depression (Table 4).
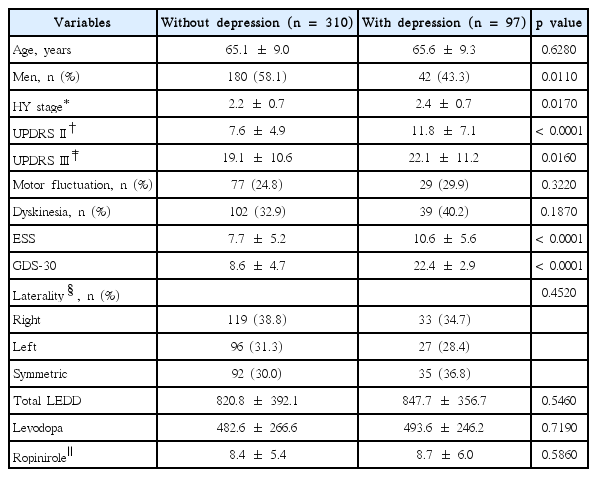
Comparison of Parkinson’s disease patients without and with depression
Multivariate logistic regression analysis showed that sex, UPDRS II, and ESS were independently associated with depression. Total LEDD, levodopa dose, and ropinirole dose were not significant risk factors (Table 5).

Depression, univariate and multivariate logistic regression analysis
Comparison of the ropinirole dose between patients without and with EDS after total LEDD stratification
Four-hundred-thirteen patients were divided into three groups according to the percentiles of total LEDD. There were larger doses of ropinirole in patients with EDS than in patients without EDS in the lowest 33rd percentile group (p = 0.009). In the other groups, the ropinirole dose was not significantly different between patients without and with EDS (Table 6).

DISCUSSION
This observational study did not find any influence of ropinirole on EDS and depression in Korean PD patients. Younger age at visit, lower activities of daily life (ADL), and depression were independent risk factors for EDS. Women, lower ADL and EDS were independent risk factors for depression.
The relationship between DAs and EDS has been controversial. In 1999, sleep attacks of ropinirole and pramipexole were first introduced [16], but later, other studies showed that there was no difference among DAs where EDS was concerned [6,17]. It was suggested that total LEDD, rather than specific DAs, might be more important in the pathogenesis of EDS [6]. The opposite results were also reported. There was no correlation found between total LEDD and EDS, and a higher levodopa dose was associated with greater vigilance [18]. In our study, the total LEDD, levodopa dose, and ropinirole dose were not associated with EDS. We do not know the exact reason why these results are contradictory. Heterogeneous populations among studies might be a reason. A variety of clinical features may affect EDS in PD. In addition to DA use, age, gender, disease severity, poor nighttime sleep, cognition, hallucination, dyskinesia, antihypertensive medications, body mass index, and pain are associated with higher EDS [19-21]. In our study, younger age, poorer ADL, and higher GDS-30 were associated with higher EDS. It is not clear whether depression is a risk factor. In our study, depression was a risk factor for EDS, but other studies reached inconsistent conclusion. One study reported that depression was correlated with severe EDS [22], but another study reported that depression was correlated with less EDS [23]. A different study showed that there was no association between depression and EDS [24]. Another possible reason was suggested: a non-dopaminergic system might be more responsible for EDS [22]. In an animal study, dopamine and serotonin played roles in the regulation of sleep and waking [25]. Therefore, studies with more comprehensive clinical features (i.e., fatigue) are needed to understand EDS [22,26].
One possible interesting finding of our study is that patients who displayed EDS had taken a larger dose of ropinirole in the lowest 33rd percentile group of total LEDD (Table 6). Considering that most patients in the lowest 33rd percentile group of total LEDD may be early PD, this observation suggests that close attention might be needed when starting ropinirole in early PD.
We did not find any effect of dopaminergic medication on depression. Only gender, ADL and EDS were risk factors for depression in PD. DAs may alleviate depressive symptoms in PD [10,27-29]. Pramipexole is known to have a direct antidepressant effect [27]. It seems that there is not sufficient evidence for the effect of ropinirole, although it has been shown to lead to some improvement of depression in various disorders, including PD [10,30,31]. In our study, there was no difference of the ropinirole dose between patients without and with depression. One possible explanation why ropinirole did not show a clear effect, unlike pramipexole, is the difference of the binding affinities for the D3 receptor among DAs [32]. Ropinirole and pramipexole are D2/D3 DAs, but pramipexole has a higher affinity for D3 receptors than ropinirole [32]. The D3 receptor is the major dopamine receptor of the mesolimbic system [29], which may be associated with behavior and mood [32].
The risk factors for depression in PD have been reported to be severe motor symptoms, disease duration, advanced disease stage, poor ADL, high LEDD, hallucination, sleep disturbance, dysautonomia, and dementia [33,34]. Our univariate analysis results showed that there were several different factors, including advanced disease stage and severe motor symptoms, between patients without depression and with depression, but in the multivariate analysis, the independent risk factors were women, lower ADL, and higher ESS. This is noteworthy for EDS. Previous studies have reported that sleep disturbances might be a risk factor for depression, but they did not check EDS [35,36].
Our study has some limitations. First, this was an observational study. We could not determine the effect of ropinirole alone on EDS and depression because enrolled patients had taken combined antiparkinsonian medications that included ropinirole and levodopa. Second, the demographics between PD patients without and with EDS were not matched. Although we adjusted these variables with multivariate logistic regression, these differences might be biased. Third, another sleep problem (i.e., REM sleep behavior disorder, insomnia) may affect EDS, but we did not check for other sleep problems.
Notes
Conflicts of Interest
The authors have no financial conflicts of interest.
Acknowledgements
This study was supported by GlaxoSmithKline Korea (study no.116404). We would like to thank anonymous reviewers for their valuable comments and suggestions, and Kang, Seung-Min (Dream CIS CRO) for statistical analysis.
All of the authors were investigators in this study and, as such, received research funding from GSK for the study and report no conflicts of interest.