Validity and Reliability Study of the Korean Tinetti Mobility Test for Parkinson’s Disease
Article information
Abstract
Objective
Postural instability and gait disturbance are the cardinal symptoms associated with falling among patients with Parkinson’s disease (PD). The Tinetti mobility test (TMT) is a well-established measurement tool used to predict falls among elderly people. However, the TMT has not been established or widely used among PD patients in Korea. The purpose of this study was to evaluate the reliability and validity of the Korean version of the TMT for PD patients.
Methods
Twenty-four patients diagnosed with PD were enrolled in this study. For the interrater reliability test, thirteen clinicians scored the TMT after watching a video clip. We also used the test-retest method to determine intrarater reliability. For concurrent validation, the unified Parkinson’s disease rating scale, Hoehn and Yahr staging, Berg Balance Scale, Timed-Up and Go test, 10-m walk test, and gait analysis by three-dimensional motion capture were also used. We analyzed receiver operating characteristic curve to predict falling.
Results
The interrater reliability and intrarater reliability of the Korean Tinetti balance scale were 0.97 and 0.98, respectively. The interrater reliability and intra-rater reliability of the Korean Tinetti gait scale were 0.94 and 0.96, respectively. The Korean TMT scores were significantly correlated with the other clinical scales and three-dimensional motion capture. The cutoff values for predicting falling were 14 points (balance subscale) and 10 points (gait subscale).
Conclusion
We found that the Korean version of the TMT showed excellent validity and reliability for gait and balance and had high sensitivity and specificity for predicting falls among patients with PD.
Gait disturbance and postural instability are cardinal features of Parkinson’s disease (PD) and detract from quality of life. Objective measurement of gait and balance to observe the progression of disease and reduce the fall risk of patients has been the subject of much attention [1]. Most clinicians assess gait and balance by relying on subjective observations during the neurological examination. Several clinical scales for gait and balance have been developed. The most commonly used scales for gait and balance status in PD are Hoehn and Yahr (H&Y) staging and the Unified Parkinson’s Disease Rating Scale (UPDRS) part III [2,3]. H&Y staging is a simple and well-known method; however, the H&Y scale is not linear and cannot even be ordered by rank [4]. The UPDRS part III contains items of gait and postural instability, but the scoring is also broad and simple. The Berg balance test, which is also widely used in estimating postural imbalance, has been validated for PD [5]. However, the Berg balance test only can estimate balance and cannot evaluate gait itself.
As a way overcome these limitations of clinical scales, the Tinetti Mobility Test (TMT), also called the Performance-Oriented Mobility Assessment, was introduced [6]. The TMT has been widely used and has been recommended as a way to assess mobility, balance, gait, and fall risk in the elderly [7]. Previous reports have demonstrated that the TMT is one of the most accurate tools for assessing patients with PD and has acceptable validity and reliability [8]. The TMT was translated into Korean in a previous study and was shown to be a reliable and valid tool for chronic stroke patients [9]. However, there has been no report of the validation of the Korean version of the TMT in PD patients.
The purpose of this study was to investigate the reliability and validity of the Korean version of the TMT in patients with PD.
MATERIALS & METHODS
This is a cross-sectional observational study. The primary goal was to evaluate the reliability and validity of the Korean version of the TMT in patients with PD. The secondary goal was to identify the most accurate TMT cutoff value for predicting falls in patients with PD. This study was approved by Interstitial Review Board in Haeundae Paik Hospital (IRB No. 2016-04-024).
Subjects
Twenty-four patients diagnosed with PD according to the Queen Square Brain Bank criteria [10] at three different hospitals were enrolled in this study. The inclusion criteria were as follows: 1) PD patients who complained of gait disturbance and postural instability, 2) patients with PD aged 50 to 80 years, 3) H&Y stage 2 to 4. All participants were given informed consent.
The exclusion criteria were as follows: 1) patients who were diagnosed with dementia, 2) patients who had an evident risk of falling while performing the test, 3) patients who had other diseases affecting gait such as neuromuscular or cardiopulmonary dysfunction, and 4) patients who were diagnosed with atypical parkinsonism.
Basic demographic factors including age, sex, disease duration, and falling history were obtained. We used the UPDRS motor scale (part III), the balance subscale (item 30), and the H&Y stage to evaluate disease severity. We obtained each patient’s falling history from an interview at baseline screening. A fall was defined as an unexpected falling event that ended with the subject coming to rest on the ground and was not due to an extrinsic event. A “faller” was defined as a person who had fallen more than once within six months [11]. We categorized the patients into faller and non-faller groups on the basis of their falling history.
Korean version of the TMT
Although a Korean TMT has been published for stroke patients, this published Korean TMT has several limitations: 1) the paper introducing the Korean TMT is written in Korean, which makes it difficult to find through online searches in PubMed or Embase; 2) the published Korean TMT includes unfamiliar term such as stance phase that are difficult to understand by the public. 3) only two examiners were used to estimate interrater reliability. Therefore, we constructed a new version of the Korean TMT according to the following method.
The TMT as tested in this study is composed of two distinct components, including a balance subscale (9 items, 16 points) and a gait subscale (8 items, 12 points). Therefore, there are 17 items, each of which is rated on a scale of 0 to 1 or 2, and the maximum possible score is 28 points. The total time taken to perform the TMT is approximately 10 minutes per participant. The translation process of the TMT is accurate and reflects Korean culture.
For the translation of the TMT into its Korean version, one movement specialist and one non-medical-expert translator participated in the translation. Subsequently, another non-medical-expert translator retranslated the Korean TMT into the English version and compared it with the original version of the TMT. Each non-medical-expert translator was a person not associated with healthcare who had lived in an English-speaking country for at least 10 years. The three people who participated in the translation collaborated to adapt it to Korean culture (Supplementary Table 1 in the online-only Data Supplement).
Checking the reliability and validity of the TMT
Three movement specialists from different hospitals discussed how to perform the TMT. All TMTs were recorded with a video camcorder with anteroposterior and mediolateral views.
For the intrarater reliability test, we used the test-retest method. We performed the TMT twice with a 30-minute interval between tests. For interrater reliability, thirteen clinicians who worked at different hospitals gathered together and scored the TMT while watching the video clips.
For concurrent validation, clinical tests for gait and balance and three-dimensional motion captures were performed. Clinical tests for gait included the Timed-up and go (TUG) test, 10-m walk test, and UPDRS part III. Clinical scales for balance and the Berg balance test were performed. For objective quantification of gait, we checked spatiotemporal parameters from the three-dimensional motion analysis.
Gait analysis by three-dimensional motion capture
To evaluate gait objectively, we used three-dimensional motion capture VICON (Oxford, UK) at a sample rate of 100 Hz for quantification of spatiotemporal parameters. The participants were asked to walk along a 6-m track under 12 infrared cameras for motion capture. Stride length, walking speed, cadence, step time, stride time, step length, single support, double support and proportion of the gait cycle spent in the stance phase were measured.
Statistics
All results were calculated using SPSS version 21 (IBM Corp., Armonk, NY, USA) and R version 3.1.2. For intra- and interrater reliability, an Interclass Correlation Coefficient (ICC) derived from a two-way random-effects model was used. For internal consistency, we calculated Cronbach’s alpha in each subscale (“irr”, “psy”, “boot” packages).
The concurrent validity of the TMT was obtained by calculating the correlation with the Berg balance test, the UPDRS balance and gait subscores, the H&Y stage, the TUG, and the 10-m walk test. Gait parameters from three-dimensional motion analyses were also compared with TMT results. Spearman correlation analysis was used to evaluate the correlation between TMT and other parameters. The level of significance was set at p < 0.05.
Receiver Operating Characteristic (ROC) analysis was performed to assess the sensitivity and specificity of the TMT score in predicting falls. An ROC curve analysis and an estimate of the area under the ROC curve (AUC) were used to assess the cutoff points for TMT in PD.
RESULTS
The demographics of the participants are shown in Table 1. Their mean age was 72.33 ± 6.95 years, and fourteen of the participants were men. The mean H&Y stage was 2.39 ± 7.37, and the mean UPDRS part III score was 15 ± 3.20. Among the 24 participants, 8 patients had a history of falling.

Demographic factors of participants
Reliability of the TMT
The results of the reliability tests for the TMT are shown in Table 2. The interrater reliability of the balance subscales ranged from 0.94 to 0.98 with an ICC of 0.97. The interrater reliability of the gait scale ranged from 0.90 to 0.97 with an ICC of 0.94. Test-retest reliability, used as a measure of intrarater reliability, was ICC = 0.97 for the balance scale and 0.96 for the gait scale. Cronbach’s alpha coefficients for the internal consistency of the Korean version of the Tinetti balance and gait scale were 0.74 and 0.72, respectively, with a confidence interval from 0.69 to 0.77 and from 0.67 to 0.76.

Reliability of the Tinetti gait and balance tests
Concurrent validity of Korean TMT
Concurrent validity compared with each clinical test is shown in Table 3. The Tinetti gait scale showed a negative correlation with the 10-m walking test (r = -0.56) and the TUG (r = -0.64). Regarding three-dimensional gait analysis, the Tinetti gate scale showed a positive correlation with stride length (r = 0.77), walking speed (r = 0.71), step length (r = 0.81) and single support (r = 0.45), and a negative correlation with stance phase and double support. The Tinetti balance scale showed a positive correlation with the Berg balance scale (r = 0.73) and a negative correlation with the TUG (r = -0.64).
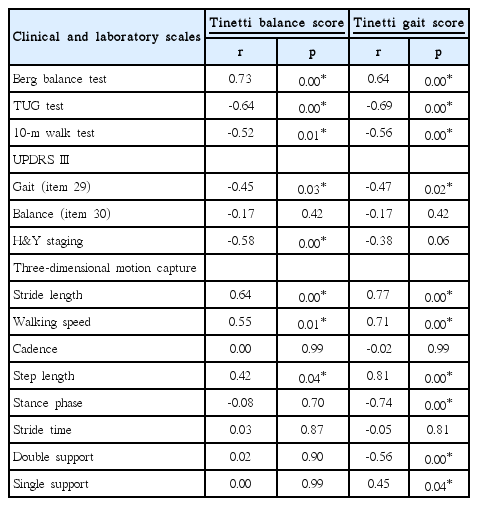
Concurrent validity of TMT with other clinical and laboratory parameters
ROC analysis to predict falling
Table 4 shows the outcomes of the ROC analysis. The Tinetti gait scale shows high sensitivity (88%) and specificity (63%) when 10 is selected as the cutoff value. The Tinetti balance scale score of 14 was selected as the cutoff with the highest sensitivity (81%) and specificity (75%) (Figure 1). The value of the AUC for predicting falls was 0.773 for the balance scale and 0.766 for the gait scale.

ROC analysis of Tinetti balance and gait scores
Receiver Operating Characteristic curve of Tinetti gait and balance scale for predicting falling in Parkinson’s disease.
DISCUSSION
Our study is the first report of the reliability and validity of the TMT for evaluating patients with PD in Korea. Furthermore, we used a number of tests, including objective estimation via three-dimensional motion capture, for concurrent validation. We found that the Korean version of the TMT showed excellent reliability and validity for patients with PD. Our results are in accordance with previous reports of its high reliability and validity for patients with PD [8]. A kappa coefficient from 0.61 to 0.80 is regarded as “substantial” reliability, and a value above 0.8 is regarded as “good” reliability [12]. In our results, the Korean version of the TMT showed excellent interrater and intrarater reliability. Our results showed higher inter- and intra-reliability and internal consistency than previously reported for the original TMT. Previous reports investigated its reliability for use by students and therapists, but our study targeted movement experts [13].
The Tinetti balance scale showed a positive correlation with clinical and laboratory balance scales. Previous studies have supported a correlation between the TMT and the Berg balance test, TUG, 10-m walking test, and H&Y stage, consistent with our results [8,14]. The Tinetti balance scale is most highly correlated with the Berg balance test and TUG. The Berg balance test is the most accurate scale for estimating balance [11]. Interestingly, the Tinetti balance scale score did not correlate with the UPDRS balance subscore (item 30) but was significantly correlated with the Tinetti gait scale score (item 29). One possible explanation is that postural imbalance in PD is episodic and inconsistent and is therefore difficult to evaluate in one trial. However, gait performance is a constant process, and balance is needed for gaiting. As shown in Table 3, gait and postural instability are closely related to each other. The measurement of balance using the UPDRS score has limitations for evaluating balance because it was checked only by the pull test.
The Tinetti gait scale also showed a strong correlation with the Berg balance test, TUG, 10-m walk test stride length, and walking speed. Objective gait parameters including stride length and walking speed showed the strongest correlation with the Tinetti gait and balance scale. A previous study demonstrated that the Tinetti gait scale was also significantly correlated with the measurements of the GAITRite (CIR system Inc., Franklin, NJ, USA) electronic system [15]. Our results demonstrated that the Korean version of the TMT was more strongly associated with gait speed and stride length than was previously reported. The 10-m walk test showed a significant but relatively weak correlation with the Korean version of the TMT.
The Tinetti balance scale was associated with H&Y stage, but the Tinetti gait scale was not. We assumed that this was because the H&Y stage is graded via laterality and postural imbalance and therefore cannot reflect gait status.
The TMT has been widely used to predict falls in the elderly [7]. We found that cutoff values of 14 points on the Tinetti balance scale and 10 points on the gait scale showed the most accurate sensitivity and specificity for predicting falls among patients with PD. Previous reports also suggested that the optimal cutoff value of the Tinetti balance scale for predicting falling was 10 points among the elderly [16,17], but for patients with PD, the cutoff total score for the original TMT was 20 points, which is lower than our result [8]. The Tinetti gait scale and balance scale showed acceptable accuracy for predicting falling in patients with PD in this study.
Our study has several limitations. First, the sample size was not large; therefore, the estimated power was low (55–62%). Further research will be needed to confirm the effect size of our study finding. Second, we did not enroll patients in an advanced stage of PD owing to their falling risk; therefore, interreliability for each item was low. Third, our study targeted only movement experts, not therapists or nurses.
In conclusion, our study demonstrated that the Korean version of the TMT has acceptable reliability and validity as an assessment tool for gait and balance among patients with PD. It is also useful for predicting falling among patients with PD using cut-off values of 14 on the balance scale and 10 on the gait scale.
Supplementary Materials
The online-only Data Supplement is available with this article at https://doi.org/10.14802/jmd.17058.
Notes
Conflicts of Interest
The authors have no financial conflicts of interest.
Acknowledgements
This research was funded by the Korean Movement Disorder Society (KMDS) as part of the “2016 Academic Research Funding” project.