1Department of Neurology, Seoul National University Hospital, Seoul, Korea
2Department of Neurology, Kyungpook National University Chilgok Hospital, School of Medicine, Kyungpook National University, Daegu, Korea
3Brain Science and Engineering Institute, Kyungpook National University, Daegu, Korea
4Department of Neurology, Kangnam Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea
Corresponding author: Jin-Sun Jun, MD Department of Neurology, Kangnam Sacred Heart Hospital, Hallym University College of Medicine, 1 Singil-ro, Yeongdeungpo-gu, Seoul 07441, Korea / Tel: +82-2-829-5125 / Fax: +82-2-847-1617 / E-mail: junjinsun0401@gmail.com
• Received: August 7, 2019 • Revised: September 10, 2019 • Accepted: September 23, 2019
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Nonketotic hyperglycemia (NKH) is characterized by elevated blood glucose levels associated with hyperosmolarity and dehydration in the absence of ketone formation [1]. NKH may produce various neurological symptoms, including an altered mentality, seizures, and involuntary movements, such as chorea and tremor [1]. Although both chorea and seizures are often observed in patients with NKH, their coexistence in these patients is extremely rare. Herein, we report a patient who concurrently developed hemichorea and seizures secondary to NKH.
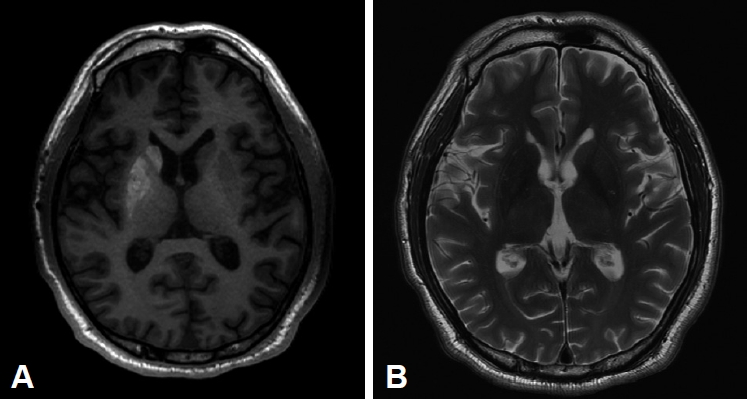
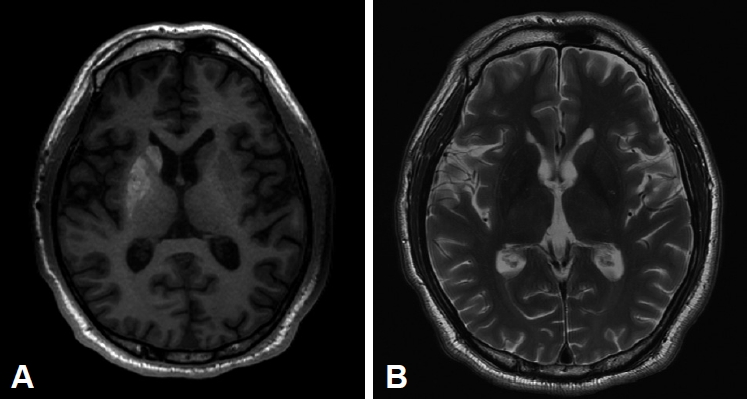
A 50-year-old man presented with involuntary abnormal movements of the left upper- and lower-limbs that had developed a few days prior to seeking treatment. He also described three episodes of loss of consciousness with diffuse tonic contractions. The patient had a 6-year history of type 2 diabetes mellitus (DM), which was poorly controlled with oral hypoglycemic agents. He had no history of movement disorders or epilepsy. At the emergency room, he showed left-sided choreiform movements, which were continuous and could not be suppressed voluntarily. Furthermore, he suddenly showed asymmetric tonic limb posturing with extension on the left side and secondary generalization, which lasted for less than 1 minute. Laboratory tests revealed a blood glucose level of 423 mg/dL, with a HbA1c of 14.6%, and the calculated serum osmolality was 290 mosm/kg. Serum ketones were negative. Magnetic resonance imaging of the brain showed an abnormally strong hyperintense signal in the right caudate and lentiform nuclei on T1-weighted images (Figure 1A) and an isointense signal on T2-weighted images (Figure 1B). Electroencephalography (EEG) revealed periodic rhythmic spike-wave discharges originating from the right temporo-occipital area without clinical signs or symptoms, suggesting subclinical seizures (Supplementary Figure 1 in the online-only Data Supplement). These epileptiform discharges were detected two or three times hourly and lasted for 20–30 seconds. He was diagnosed with NKH-induced hemichorea and seizures. He was started on insulin therapy with fluid replacement. On day 1, his choreiform movements persisted (Supplementary Video 1 in the online-only Data Supplement). On day 4, the patient’s serum glucose levels were maintained to below 200 mg/dL and his involuntary movements improved gradually. Follow-up EEG on day 7 did not reveal any epileptiform discharges. The patient was discharged on day 10 after his symptoms had resolved completely.
The clinical, laboratory, electrophysiological, and brain imaging findings of our patient strongly suggested NKH-related chorea and seizures. To the best of our knowledge, this is the second case report of combined chorea and seizures in a patient with NKH. Chung et al. [2] first reported the co-occurrence of these symptoms due to NKH. Interestingly, the previous case showed hemichorea with focal seizures of temporo-occipital onset, which is consistent with our case.
Chorea related to NKH is mainly observed in elderly Asian women with type 2 DM [3,4]. In a meta-analysis including 53 NKH-associated chorea patents, more than 80% of the patients showed hemichorea with contralateral putaminal hyperintensity [3], which is in agreement with our case. Although typical neuroleptic drugs and sometimes benzodiazepines are needed for the management of chorea in many NKH cases [3,5], this abnormal movement can be treated only with appropriate control of blood glucose levels, which is supported by our findings. In the abovementioned meta-analysis, 16 patients were also treated only with blood glucose control and showed complete remission within 1 month after symptom onset [3]. The favorable prognosis of chorea in our patient may be attributed to the relatively young age at onset. Lee et al. [5] reported that older age was the sole significant predictor for the persistence of glycemic chorea/ballism one month after onset, and the mean age (standard deviation) of glycemic chorea/ballism patients in their study was 69.8 (13.2) years.
It is known that seizures due to hypoglycemia are mainly generalized, whereas seizures due to hyperglycemia are commonly focal in nature [6]. The most frequent type of seizures due to hyperglycemia are motor seizures in the form of epilepsia partialis continua [6]. NKH-related seizures are generally resistant to antiepileptic drugs but respond to the correction of glucose levels and appropriate fluid replacement [6].
The pathophysiology of chorea and seizures related to NKH is not well understood. One possible mechanism is that hyperglycemia-induced autoregulatory dysfunction leads to hypoperfusion and subsequent activation of anaerobic metabolism. This condition results in a decreased level of gamma-aminobutyric acid, which may not only cause basal ganglia dysfunction but also lower the threshold for seizure activity. Another possible mechanism is that hyperviscosity resulting from hyperglycemia causes vascular insufficiency that provokes transient dysfunction of the basal ganglia and some cortical regions. However, these hypotheses could not explain why, unlike seizures, chorea generally persists after normalization of glucose levels, and this phenomenon needs to be further investigated. A recent study using transcranial magnetic stimulation showed that hyperglycemic hemichorea is related to increased inhibitory activity in the motor cortex [7]. This finding may reflect a compensatory mechanism to reduce the severity of symptoms.
Video 1. The pattern of involuntary movements was continuous, arrhythmic, and dance-like and were confined to left upper and lower limbs.
Notes
Conflicts of Interest
The authors have no conflicts of interest or financial support to report.
Author Contributions
Conceptualization: Ryul Kim and Jin-Sun Jun. Data curation: Hee-Jin Cho and Jin-Sun Jun. Visualization: Ryul Kim. Writing—original draft: Ryul Kim. Writing—review & editing: Ho-Won Lee and Jin-Sun Jun.
Figure 1.
Brain magnetic resonance imaging (MRI) findings. A: MRI revealed increased signal intensities in the right caudate and lentiform nuclei in T1-weighted axial imaging. B: There were no significant signal abnormalities in T2-weighted axial imaging.
REFERENCES
1. Borensztein A, Walker RH, Schell R, Guber HA. Hyperglycemia-induced involuntary movements: 2 case reports and a review of the literature. AACE Clinical Case Rep 2015;1:e165–e169.Article
2. Chung SJ, Lee JH, Lee SA, No YJ, Im JH, Lee MC. Co-occurrence of seizure and chorea in a patient with nonketotic hyperglycemia. Eur Neurol 2005;54:230–232.ArticlePubMed
3. Oh SH, Lee KY, Im JH, Lee MS. Chorea associated with non-ketotic hyperglycemia and hyperintensity basal ganglia lesion on T1-weighted brain MRI study: a meta-analysis of 53 cases including four present cases. J Neurol Sci 2002;200:57–62.ArticlePubMed
4. Lee SH, Shin JA, Kim JH, Son JW, Lee KW, Ko SH, et al. Chorea-ballism associated with nonketotic hyperglycaemia or diabetic ketoacidosis: characteristics of 25 patients in Korea. Diabetes Res Clin Pract 2011;93:e80–e83.ArticlePubMed
5. Lee D, Kwon YN, Shon SH, Lee JH, Ahn TB. Glycemic and vascular choreoballism as main causes of secondary choreoballism involving the putamen. Parkinsonism Relat Disord 2016;30:29–35.ArticlePubMed
6. Moien-Afshari F, Téllez-Zenteno JF. Occipital seizures induced by hyperglycemia: a case report and review of literature. Seizure 2009;18:382–385.ArticlePubMed
7. Li JY, Chen R. Increased intracortical inhibition in hyperglycemic hemichorea‐hemiballism. Mov Disord 2015;30:198–205.ArticlePubMed
Figure & Data
References
Citations
Citations to this article as recorded by
Diabetic striatopathy and other acute onset de novo movement disorders in hyperglycemia Subhankar Chatterjee, Ritwik Ghosh, Payel Biswas, Shambaditya Das, Samya Sengupta, Souvik Dubey, Biman Kanti Ray, Alak Pandit, Julián Benito-León, Rana Bhattacharjee Diabetes & Metabolic Syndrome: Clinical Research & Reviews.2024; 18(3): 102997. CrossRef
Oxidative stress: a common imbalance in diabetes and epilepsy Karen Paola Ramos-Riera, Francisca Pérez-Severiano, María Leonor López-Meraz Metabolic Brain Disease.2023; 38(3): 767. CrossRef
Recurrent Facial Focal Seizures With Chronic Striatopathy and Caudate Atrophy—A Double Whammy in an Elderly Woman With Diabetes Mellitus Subhankar Chatterjee, Ritwik Ghosh, Umesh Kumar Ojha, Diksha, Payel Biswas, Julián Benito-León, Souvik Dubey The Neurohospitalist.2022; 12(1): 147. CrossRef
Is diabetic striatopathy the culprit of seizures in a patient with ketotic hyperglycemia-induced hemichorea–hemiballismus? Abeer Sabry Safan, Omna Sharma, Muna Almasri, Ashton Ian D’Souza, Omer Suliman BMC Neurology.2022;[Epub] CrossRef
Bilateral striatum with high-signal intensity on T1-weighted MRI: A case of hemichorea induced by nonketotic hyperglycemia Yuanyi Pan, Fattyang Chew, Rongping Wang, Xuntao Yin, Yaying Li Radiology Case Reports.2021; 16(4): 895. CrossRef
 E-submission
E-submission
 , Hee-Jin Cho2
, Hee-Jin Cho2
 PubReader
PubReader ePub Link
ePub Link Cite
Cite