E-submission
E-submission
Articles
- Page Path
- HOME > J Mov Disord > Volume 13(2); 2020 > Article
-
Brief communication
Sedentary Time is Associated with Worse Attention in Parkinson’s Disease: A Pilot Study -
Sara B. W. Troutman1
 , Kirk I. Erickson2, George Grove2, Andrea M. Weinstein3,4
, Kirk I. Erickson2, George Grove2, Andrea M. Weinstein3,4 -
Journal of Movement Disorders 2020;13(2):146-149.
DOI: https://doi.org/10.14802/jmd.20015
Published online: May 29, 2020
1Department of Psychology, Pennsylvania State University, University Park, PA, USA
2Department of Psychology, University of Pittsburgh, Pittsburgh, PA, USA
3Department of Psychiatry, University of Pittsburgh, Pittsburgh, PA, USA
4The University of Pittsburgh Medical Center, Pittsburgh, PA, USA
- Corresponding author: Andrea M. Weinstein, PhD Department of Psychiatry, University of Pittsburgh, Room 464 Thomas Detre Hall, Pittsburgh 15213, PA, USA / Tel: +1-412-246-5729 / Fax: +1-412-586-9111 / E-mail: amw140@pitt.edu
Copyright © 2020 The Korean Movement Disorder Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Objective
- Cognitive symptoms of Parkinson’s disease (PD) may be alleviated by moderate-to-vigorous physical activity (MVPA), but no published research has characterized the relationship between objectively measured sedentary behavior and cognitive symptoms of PD. Therefore, the objective of this study was to assess the cross-sectional relationship between sedentary time and cognitive performance in a small pilot sample of individuals with mild-to-moderate PD.
-
Methods
- Objective measures of sedentary time were obtained using an armband accelerometer. Cognition was assessed with the Parkinson’s Disease Cognitive Rating Scale and a computerized task-switching paradigm.
-
Results
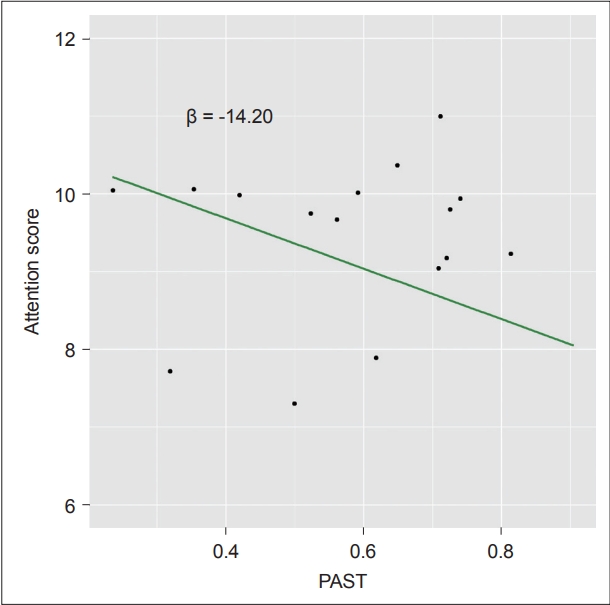
- The percentage of awake time spent in sedentary activities was negatively correlated with attention (β = -14.20, t(12) = -2.47, p = 0.03) but not other cognitive domains (p > 0.05) after controlling for MVPA and medication dosage.
-
Conclusion
- Sedentary activity may have unique associations with cognition, particularly attention, over and above MVPA in individuals with PD.
- Standard protocol approvals, registrations, and patient consents
- This study was approved by the University of Pittsburgh Institutional Review Board (PRO14020309), and all participants provided informed consent documented by their signature on consent forms.
- Participants
- Participants were recruited from the University of Pittsburgh Movement Disorders Clinic registry for a cross-sectional study. Individuals were eligible if they were between the ages of 50 and 80, fluent in English, had a diagnosis of idiopathic PD, and had a stable medication regimen. Exclusion criteria included self-reported neurological or psychological conditions (outside of PD symptoms), physical activity contraindications such as significant cardiovascular disease or conditions limiting ambulation (Supplementary Material in the online-only Data Supplement), simultaneous participation in another physical activity study, and magnetic resonance imaging contraindications (due to eligibility for another study). We did not access medical records for study participants and instead relied on self-reports of neurologic, vascular, or psychiatric illness (e.g., dementia, multiple sclerosis, etc.). Participants reported having few depressive symptoms on the Center for Epidemiological Studies Depression Scale (CES-D; average = 8.85, SD = 5.86). Any participants who scored below 22 on the Montreal Cognitive Assessment (MoCA) [13] were excluded due to significant cognitive impairment. Participants completed assessments while in the “ON” phase of their medication schedules (i.e., within 1–2 hours of ingesting medications), such that assessments reflected participants’ medication-adjusted performance.
- Cognitive assessments
- Inclusion based on the level of overall cognitive ability was determined using the MoCA. Cognitive domains that have been shown to decline in PD, including memory, working memory, verbal fluency, and attention, were assessed using the Parkinson’s Disease-Cognitive Rating Scale (PD-CRS). The immediate and delayed verbal memory measures were averaged to provide a composite score for memory (memory composite) [14]. Averaging the memory composite and attention scores created a measure of overall cognitive function, per PD-CRS recommendations (global cognition). Participants also completed a computerized task-switching paradigm to measure cognitive flexibility. In this paradigm, a single number (one to nine, excluding five) was presented and surrounded by either a circle or a square. If the number was surrounded by a circle, participants were asked to indicate whether the number was odd or even. If the number was surrounded by a square, participants were to indicate if the number was greater than or less than five. Each trial would either be the same (i.e., repeat trial) or different (i.e., switch trial) as the preceding trial. The difference between reaction time in repeat and switch trials provides a measure of local switch cost. Higher scores on this measure (greater switching costs) indicate poorer cognitive flexibility
- Physical activity measures
- Participant’s activity levels were measured for 7–10 days using a Sensewear Pro armband (Body Media Inc., Sensewear Version 7.0, Pittsburgh, PA, USA). Consistent with field standards, data were included if participants had at least 72 hours of usable data [15]. The Sensewear armband uses a proprietary algorithm to calculate METs and has been externally validated using a variety of methods [16]. The armband collected data such as number of steps, sleep time, and energy expenditure continuously in 1-minute epochs. In line with field standards, observations were classified as sedentary behavior if energy expenditure was below 1.5 METS, light activity if expenditure was between 1.5 and 3 METS, and MVPA if expenditure was 3 or more METS [10]. For all three behavior types (i.e., sedentary, light, and MVPA), we counted the total minutes in each category and calculated the percentage of awake time spent in each state by dividing the total minutes amassed for each category by the total minutes of awake time.
- Data analysis
- Local switch cost on the task-switching paradigm, memory composite, attention, and global composite were dependent variables in four separate linear regression models. Predictor variables included the primary variable of interest, namely, percent awake sedentary time (PAST; total number of minutes in sedentary time divided by total number of awake minutes); PD medication dosage (LED) [17] was used as a proxy variable, controlling for disease stage and age; and percent MVPA time (PMVPA; total number of minutes in MVPA divided by the total number of awake minutes) was used to control for the effects of MVPA. Significance was set at p = 0.05.
PATIENTS AND METHODS
- Participants
- After an initial screening of 84 individuals in mild-to-moderate PD stages (i.e., Hoehn & Yahr score of 1–2) [1], 20 participants met the criteria. Two participants dropped out for unknown reasons, one had a MoCA score of < 22 points; thus, 17 participants successfully enrolled in the study (female = 3; White, non-Hispanic = 17; average age = 65.07; average UPDRS motor score = 20.26) (Supplementary Table 1 in the online-only Data Supplement). Of these 17 participants, one could not learn the task-switching paradigm and was excluded from task-switching analyses. Both men and women were recruited, but since PD is most prevalent in Caucasian men [18], this demographic group was most represented in the registry and in the final sample.
- Cognitive measures
- Controlling for the effect of PMVPA and LED, PAST was negatively correlated with attention (Table 1, Figure 1). Task-switching, memory, and global cognition were not significantly related to PAST. PMVPA and LED were not significantly related to any cognitive measures.
RESULTS
- This pilot study provides evidence linking sedentary behaviors (PAST) and attention independent of the effect of percent time spent in moderate-to-vigorous physical activity (PMVPA). As expected, participants who spent more of their waking hours in sedentary time showed worse attention. This effect was overand above- MVPA, suggesting that the relationship between sedentary behavior and cognition is different than the relationship between MVPA and cognition. This link between sedentary behavior and attention is consistent with previous evidence suggesting that sedentary behavior is associated with poorer cognitive performance in healthy individuals, independent of physical activity [12]. Thus, the current findings extend this relationship to individuals with PD. Inconsistent with previous literature, however, we found no evidence linking sedentary behavior and task-switching, memory, or overall cognitive performance.
- This pilot trial has implications for our understanding of the difference between sedentary behavior and physical activity. Physical activity is positively associated with task-switching, memory, attention, and overall cognition [2,3]. If inactivity was simply the inverse of physical activity, we would expect inactivity to lead to worse outcomes on all of these measures, which is not what we found. Moreover, MVPA was not associated with cognition in this sample. This could be because this sample was very inactive, thus limiting MVPA variability. With only 17 participants, this study only had enough power to detect very large effects (f2 = 0.71), which may explain the null association between sedentary behavior and attention, memory, or overall cognition. Moreover, the significant relationships observed in this study would not survive a Bonferroni correction (p > 0.01). Even so, these results suggest that, relative to other aspects of cognition, sedentary behavior may be independently related to attention over and above MVPA in individuals with PD.
- It is likely that our results are not purely an artifact of disease stage and age of the participant. We accounted for these possibilities by covarying for the effect of LED, which has been shown to be a statistical proxy for disease stage and age in PD [17]. Moreover, this sample did not include individuals with motor complications that precluded their ability to exercise or individuals with other comorbid pathologies (e.g., multiple sclerosis, dementia; Supplementary Table 1 in the online-only Data Supplement). Still, these results represent a contribution to the literature, as individuals with PD spend more time in sedentary behavior than individuals without PD [19]. The finding that sedentary behavior is independent of MVPA in predicting attention ability indicates the need for future intervention studies to focus not simply on increasing physical activity but also on the potential contribution of reducing sedentary time. In short, this pilot study points to the need to further study the consequences of sedentary behavior in individuals with PD.
DISCUSSION
Supplementary Materials
-
Conflicts of Interest
The authors have no financial conflicts of interest.
-
Author Contributions
Conceptualization: Sara B. W. Troutman, Andrea M. Weinstein, and Kirk I. Erickson. Data curation: Sara B. W. Troutman, Andrea M. Weinstein, and George Grove. Formal analysis: Sara B. W. Troutman and Andrea M. Weinstein. Funding acquisition: Andrea M. Weinstein and Kirk I. Erickson. Methodology: all authors. Project administration: Andrea M. Weinstein. Visualization: Sara B. W. Troutman. Writing-original draft: Sara B. W. Troutman and Andrea M. Weinstein. Writing-review & editing: George Grove and Kirk I. Erickson.
Notes
- We thank the staff and students of the Brain Aging and Cognitive Health lab at the University of Pittsburgh, the Language and Aging Lab at the Pennsylvania State University, and the Center for Healthy Aging at the Pennsylvania State University for their support of this work. We also thank Michele T. Diaz, PhD for her helpful feedback on the writing.
- This project was funded by National Institutes of Health (NIH) grants P30 AG024827 (KIE), F31NS089111 (AMW), and T32-AG049676 (SBWT).
Acknowledgments

- 1. Hoehn MM, Yahr MD. Parkinsonism: onset, progression and mortality. Neurology 1967;17:427–442.ArticlePubMed
- 2. Tanaka K, Quadros AC Jr, Santos RF, Stella F, Gobbi LT, Gobbi S. Benefits of physical exercise on executive functions in older people with Parkinson’s disease. Brain Cogn 2009;69:435–441.ArticlePubMed
- 3. Bocquillon P, Bourriez JL, Palmero-Soler E, Defebvre L, Derambure P, Dujardin K. Impaired early attentional processes in Parkinson’s disease: a high-resolution event-related potentials study. PLoS One 2015;10:e0131654.ArticlePubMedPMC
- 4. Loprinzi PD, Edwards MK, Crush E, Ikuta T, Del Arco A. Dose-response association between physical activity and cognitive function in a national sample of older adults. Am J Health Promot 2018;32:554–560.ArticlePubMed
- 5. Colcombe SJ, Erickson KI, Scalf PE, Kim JS, Prakash R, McAuley E, et al. Aerobic exercise training increases brain volume in aging humans. J Gerontol A Biol Sci Med Sci 2006;61:1166–1170.ArticlePubMedPDF
- 6. Prakash RS, Voss MW, Erickson KI, Kramer AF. Physical activity and cognitive vitality. Annu Rev Psychol 2015;66:769–797.ArticlePubMed
- 7. Petzinger GM, Fisher BE, McEwen S, Beeler JA, Walsh JP, Jakowec MW. Exercise-enhanced neuroplasticity targeting motor and cognitive circuitry in Parkinson’s disease. Lancet Neurol 2013;12:716–726.ArticlePubMedPMC
- 8. Loprinzi PD, Danzl MM, Ulanowski E, Paydo C. A pilot study evaluating the association between physical activity and cognition among individuals with Parkinson’s disease. Disabil Health J 2018;11:165–168.ArticlePubMed
- 9. da Silva FC, Iop RDR, de Oliveira LC, Boll AM, de Alvarenga JGS, Gutierres Filho PJB, et al. Effects of physical exercise programs on cognitive function in Parkinson’s disease patients: a systematic review of randomized controlled trials of the last 10 years. PLoS One 2018;13:e0193113.ArticlePubMedPMC
- 10. Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, et al. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc 2000;32(9 Suppl):S498–S504.ArticlePubMed
- 11. Ainsworth BE, Haskell WL, Leon AS, Jacobs DR Jr, Montoye HJ, Sallis JF, et al. Compendium of physical activities: classification of energy costs of human physical activities. Med Sci Sports Exerc 1993;25:71–80.ArticlePubMed
- 12. Kesse-Guyot E, Andreeva VA, Lassale C, Hercberg S, Galan P. Clustering of midlife lifestyle behaviors and subsequent cognitive function: a longitudinal study. Am J Public Health 2014;104:e170–e177.ArticlePubMedPMC
- 13. Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc 2005;53:695–699.ArticlePubMed
- 14. Pagonabarraga J, Kulisevsky J, Llebaria G, García-Sánchez C, Pascual-Sedano B, Gironell A. Parkinson’s disease-cognitive rating scale: a new cognitive scale specific for Parkinson’s disease. Mov Disord 2008;23:998–1005.ArticlePubMed
- 15. Tian Q, Glynn NW, Erickson KI, Aizenstein HJ, Simonsick EM, Yaffe K, et al. Objective measures of physical activity, white matter integrity and cognitive status in adults over age 80. Behav Brain Res 2015;284:51–57.ArticlePubMedPMC
- 16. Santos-Lozano A, Hernández-Vicente A, Pérez-Isaac R, Santín-Medeiros F, Cristi-Montero C, Casajús JA, et al. Is the SenseWear Armband accurate enough to quantify and estimate energy expenditure in healthy adults? Ann Transl Med 2017;5:97.ArticlePubMedPMC
- 17. Tomlinson CL, Stowe R, Patel S, Rick C, Gray R, Clarke CE. Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov Disord 2010;25:2649–2653.ArticlePubMed
- 18. Wright Willis A, Evanoff BA, Lian M, Criswell SR, Racette BA. Geographic and ethnic variation in Parkinson disease: a population-based study of US Medicare beneficiaries. Neuroepidemiology 2010;34:143–151.ArticlePubMedPMC
- 19. Benka Wallén M, Franzén E, Nero H, Hagströmer M. Levels and patterns of physical activity and sedentary behavior in elderly people with mild to moderate Parkinson disease. Phys Ther 2015;95:1135–1141.ArticlePubMedPDF
REFERENCES
Figure & Data
References
Citations
- A systematic review of the associations between sedentary behavior, physical inactivity, and non-motor symptoms of Parkinson’s disease
Aiza Khan, Joy Ezeugwa, Victor E. Ezeugwu, Michael Francis Salvatore
PLOS ONE.2024; 19(3): e0293382. CrossRef - A blood-based marker of mitochondrial DNA damage in Parkinson’s disease
Rui Qi, Esther Sammler, Claudia P. Gonzalez-Hunt, Ivana Barraza, Nicholas Pena, Jeremy P. Rouanet, Yahaira Naaldijk, Steven Goodson, Marie Fuzzati, Fabio Blandini, Kirk I. Erickson, Andrea M. Weinstein, Michael W. Lutz, John B. Kwok, Glenda M. Halliday, N
Science Translational Medicine.2023;[Epub] CrossRef
Comments on this article
 PubReader
PubReader ePub Link
ePub Link Cite
Cite