Department of Neurology, College of Medicine, The Catholic University of Korea, Seoul, Korea
Corresponding author: Joong-Seok Kim, MD, PhD Department of Neurology, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 222 Banpo-daero, Seocho-gu, Seoul 06591, Korea / Tel: +82-2-2258-6078 / Fax: +82-2-599-9686 / E-mail: neuronet@catholic.ac.kr
• Received: January 13, 2021 • Revised: May 24, 2021 • Accepted: July 29, 2021
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Athletes can develop task-specific dystonia, which is referred to as “yips.” Athlete dystonia has been reported in a variety of sports, including golf, ping pong, tennis, archery, darts, shooting, pitching, and running [1-6]. Recently, a case of billiard-related dystonia was reported [7]. In billiards, the player uses a cue stick to strike a ball on the billiard table to make it hit other balls. The player usually sets the stick on his or her nondominant hand to stabilize it and then moves the stick with the dominant arm. Here, we present a 52-year-old professional billiard player who experienced an awkward feeling in his right arm exclusively while playing billiards.
The patient was right-handed and had been a professional billiard player for 30 years. He practiced every day with his right hand handling the stick. Five years prior to his visit, he had difficulty aiming the ball while moving the right arm to strike the ball. He described his arm being ‘locked’ when he tried to strike a ball extending his elbow (Figure 1A-C). This forced his arm to hesitate a moment just before the impact of striking, causing a subtle disturbance of fluent arm movement (Supplementary Video 1 in the online-only Data Supplement). He did not have a relevant medical history and denied exposure to any medications, including neuroleptics. The patient never suffered any orthopedic problems with his limbs and did not have any family members with hyperkinetic or hypokinetic disorders.
Neurological examination did not reveal any abnormalities. Spontaneous posture or tremor was not observed, and his muscle tone was normal. The task-specific dystonia was not distracted or entrained to the examiner’s instructions, such as mental distraction. He did not describe any pain that might have caused the symptoms. Laboratory examinations, including measurements of serum ceruloplasmin, copper levels, thyroid function, and biochemical screenings, were unremarkable. Brain magnetic resonance imaging did not display any abnormalities. A genetic study of DYT1 in the torsion A gene and whole-exome sequencing did not find any abnormalities.
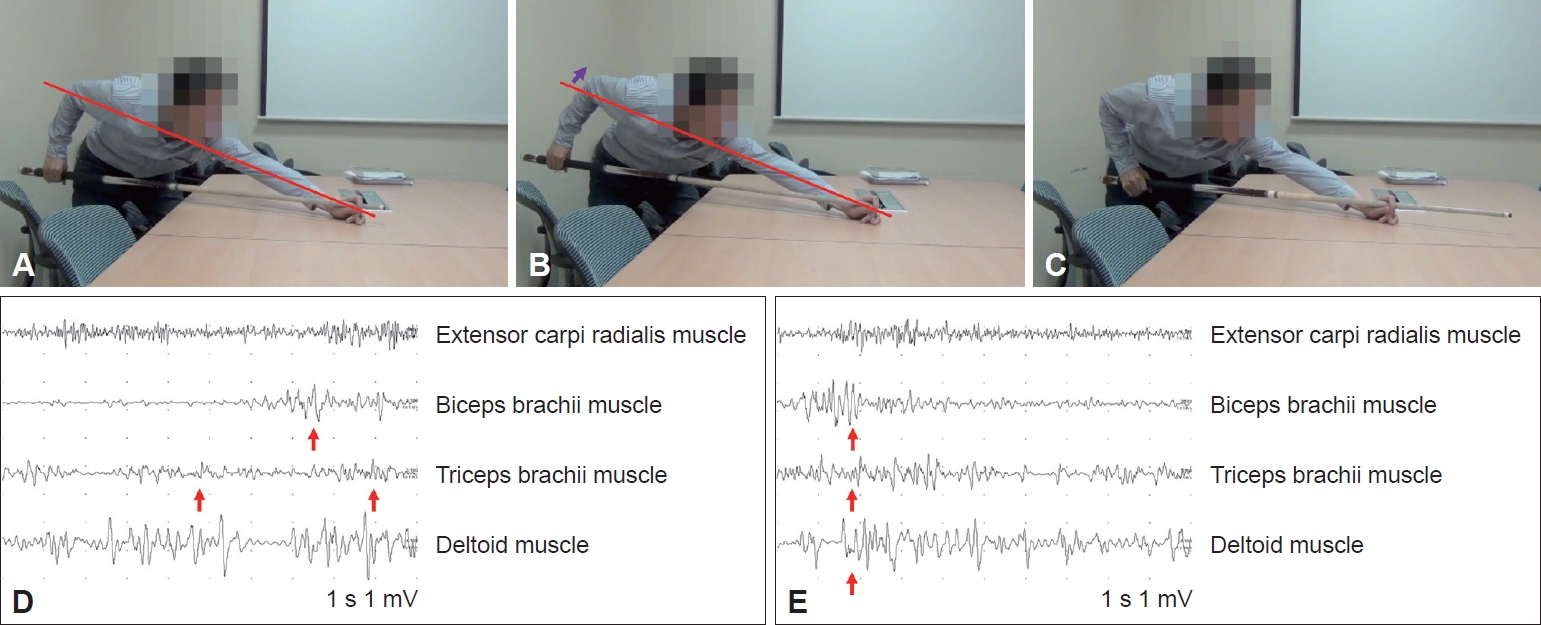
Surface electromyography (EMG) was conducted to provide electrophysiologic evidence of dystonia. EMG leads were attached in the external carpi radialis, biceps, triceps, and deltoids of the right upper limb. In the resting position, there were no subclinical activations of the recorded muscles. During to-and-fro movements of the right arm without cue sticks, alternating activation of the biceps and triceps muscles was found. Abnormal cocontractions or oscillatory muscle activations were not observed (Figure 1D). However, during the same movement with the cue stick, triceps and deltoids cocontracted immediately after bicep contraction when pulling the cue backward (Figure 1E). This precipitated the patient’s feeling of his arm being locked during the strike. There was no pattern of overflow or alleviating maneuver to smooth the impact of hitting a ball.
Treatment with a beta-blocker (propranolol), a benzodiazepine, and anticholinergics was attempted but did not alleviate his symptoms. Botulinum A toxin injection was performed. Because this was a task-specific and nonfixed form of dystonia, muscles relevant to the sport were meticulously selected. The right biceps, triceps, brachioradialis, and extensor carpi radialis muscles were injected with botulinum A toxin at 20, 20, 15, and 15 IU, respectively. The patient was not satisfied with the treatment and refused further botulinum A toxin treatment. His symptoms were followed at regular periods for 18 months but did not progress. He did not complain of significant difficulty with other daily activities but had to train himself to move the stick with his left arm.
The patient showed typical task-specific dystonia exclusively playing billiards. Other possible etiologies, such as neurodegenerative disease presenting as task-specific dystonia and functional dystonia, were excluded. That he presented with symptoms five years prior to his visit also argued against the possibility that his movement was an initial symptom of neurodegenerative disease because his symptom duration was sufficient for the disease to progress and present with other symptoms. His illness remained confined to the exact task and body parts. In addition, brain magnetic resonance imaging was unremarkable.
Although writer’s cramp and musician’s dystonia are the most well-known forms of task-specific dystonia, athletes’ dystonia or cramp has attracted little research attention. Many athletes simply regard this phenomenon as yips, but various sporting activities are reported to be associated with task-specific dystonia. The pathophysiology of athletes’ dystonia is poorly understood; however, overuse or overcompensation, in addition to genetic predisposition, have been suggested to influence the development of dystonia [6]. Recently, a 57-year-old man with abnormal posturing of the right upper limb was reported and his symptom occurred exclusively while playing carambole billiards [7]. He suffered movement arrest when he prepared to hit a ball. Our case is an additional report of billiard-related dystonia, but it differs in that our patient was a professional billiard player, while the previous patient only played recreationally. Although our patient showed more subtle symptoms than the patient in the other report, the impact of dystonia on his daily life was tremendous and interfered with his profession as a player. A variety of treatments were conducted but were not sufficient to enable the patient to play billiards with his right arm again. Attempts to alleviate his dystonia need to be continued and could include combinations of drugs or another regimen of botulinum A toxin injection reflecting the sports kinetics.
The patient was instructed to play with a billiard cue stick. During to-and-fro movements of the right arm with cue sticks, shoulder overextension backward was observed. This abnormal contraction was not found in the left arm in the same movement.
Notes
Ethics Statement
The Institutional Review Board at Seoul St. Mary’s Hospital approved this case report (KC21ZASI0312). The patient has consented to the submission of the case report to the journal.
Conflicts of Interest
The authors have no financial conflicts of interest.
Funding
None.
Author Contributions
Conceptualization: Joong-Seok Kim. Data curation: all authors. Formal analysis: all authors. Supervision: Joong-Seok Kim. Validation: all authors. Visualization: all authors. Writing—original draft: Hyukje Lee. Writing—review & editing: Sang-Won Yoo, Joong-Seok Kim.
Figure 1.
A-C: Schematic photos of the patient. In the last step of hitting the billiard ball, shoulder overextension backward was observed, and the patient described his arm as being ‘locked.’ The angle between the red line connecting the right elbow to the left hand and the table, which was supposed to be fixed, became widened due to cocontraction of the triceps and deltoid muscles (purple arrow). D, E: Surface electromyography (EMG) findings of the patient. EMG leads were attached in the external carpi radialis, biceps, triceps, and deltoids of the right upper limb. D: During to-and-fro movements of the right upper limb without the stick, the right extensor carpi radialis muscle manifested continuous muscle contraction due to wrist extension. Alternating activation of the biceps and triceps muscles was found. Neither abnormal cocontractions nor oscillatory muscle activations in the biceps and triceps muscles were found (red arrows). E: During to-and-fro movement of the right arm with a billiard cue stick, triceps and deltoids cocontracted immediately after bicep contraction when pulling the cue backward (red arrows). This coincided with the patient’s feeling of his arm being locked during the strike.
REFERENCES
1. Stahl CM, Frucht SJ. Focal task specific dystonia: a review and update. J Neurol 2017;264:1536–1541.ArticlePubMed
2. Frucht SJ. Billiards-related dystonia: a new task-specific dystonia. Parkinsonism Relat Disord 2019;60:12–13.ArticlePubMed
3. Nakane S, Ando Y, Matsuo H. Yips preceding baseball-related dystonia. Parkinsonism Relat Disord 2018;50:128–129.ArticlePubMed
5. Le Floch A, Vidailhet M, Flamand-Rouvière C, Grabli D, Mayer JM, Gonce M, et al. Table tennis dystonia. Mov Disord 2010;25:394–397.ArticlePubMed
6. Adler CH, Temkit M, Crews D, McDaniel T, Tucker J, Hentz JG, et al. The yips: methods to identify golfers with a dystonic etiology/golfer’s cramp. Med Sci Sports Exerc 2018;50:2226–2230.ArticlePubMed
7. Smilowska K, Domingos J, Pasman JW, van Wamelen DJ, van de Warrenburg BP, Bloem BR. Billiards-related dystonia: a new task-specific dystonia. Parkinsonism Relat Disord 2019;60:10–11.ArticlePubMed
Figure & Data
References
Citations
Citations to this article as recorded by
Analysis of arm, back and leg strength on the quality of power control in billiard sports Heryanto Nur Muhammad, Noortje Anita Kumaat, Nurkholis Nurkholis, Nur Ahmad Arief, Lutfhi Abdil Khuddus, Novadri Ayubi Health, sport, rehabilitation.2024; 10(1): 20. CrossRef
Long-Term Muscular Atrophy and Weakness Following Cessation of Botulinum Toxin Type A Injections in the Flexor Digitorum Muscle of Musicians with Focal Hand Dystonia Christos I. Ioannou, Franziska L. Hodde-Chriske, Eckart Altenmüller Toxins.2023; 15(4): 296. CrossRef
Abnormal movements “Motare” in Kyudo have the characteristics of task—specific focal dystonia Taichi Ogiso, Yoya Ono, Saiki Suzuki, Takayoshi Shimohata Rinsho Shinkeigaku.2023; 63(8): 532. CrossRef
It's in the game: A review of neurological lesions associated with sports Mariana Pedrosa, Bárbara Martins, Rui Araújo Journal of the Neurological Sciences.2023; 455: 122803. CrossRef
Function and dysfunction of the dystonia network: an exploration of neural circuits that underlie the acquired and isolated dystonias Jason S. Gill, Megan X. Nguyen, Mariam Hull, Meike E. van der Heijden, Ken Nguyen, Sruthi P. Thomas, Roy V. Sillitoe Dystonia.2023;[Epub] CrossRef
Blacksmith’s Dystonia Is Another Task-Specific Dystonia: From Past to Present Min Seung Kim, Don Gueu Park, Jung Han Yoon Journal of Movement Disorders.2022; 15(3): 284. CrossRef
 E-submission
E-submission
 , Sang-Won Yoo
, Sang-Won Yoo

 PubReader
PubReader ePub Link
ePub Link Cite
Cite