Letter to the editor Acute Extrapyramidal Side Effects Following Domperidone Intake in a 48-Year-Old Female Patient: The First Genetic Alteration and Drug Interaction Characterized
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Domperidone, a peripheral and central dopamine receptor antagonist with gastroprokinetic and antiemetic effects, is a widely prescribed medication in clinical practice. This agent presents very low rates of extrapyramidal side effects due to its negligible penetration through the blood–brain barrier (BBB) [1]. Extrapyramidal symptoms after domperidone usage have only been reported in children, adolescents and individuals with comorbidities thought to alter BBB permeability. In this report, we describe a case of a 48-year-old female with a normal medical history who displayed tongue tremor following administration of the recommended dose of domperidone. We also discuss the factors that might facilitate extrapyramidal manifestation from genetics and drug interaction perspectives.
A 48-year-old female patient without a significant medical history was admitted to our outpatient clinic with spontaneous involuntary movements of the jaw, lips and tongue muscles, which led to difficulties in chewing, speaking and swallowing. She reported that the symptoms (dominantly tongue tremor) appeared soon after she took esomeprazole (40 mg per day) and domperidone (20 mg per day) for the treatment of gastritis (Supplementary Video 1 in the online-only Data Supplement). Mild abdominal gaseous distension was found, but there was no localized abdominal pain. Apart from the abovementioned symptoms, no localized neurological symptoms, meningeal irritation or other signs were observed. Common blood biochemistry tests, urine analysis and complete blood count were unremarkable. Furthermore, cerebral magnetic resonance imaging with contrast was negative for central nervous system (CNS) damage. Subsequently, the diagnosis of domperidone-induced tongue tremor was established. Domperidone was discontinued immediately, and trihexyphenidyl was prescribed. Within 48 hours, her lingual tremor improved, and abnormal movements disappeared, which strengthened the established diagnosis of drug-induced extrapyramidal side effects. After discharge, no recurrence was observed during the three-month follow-up visits. Genetic analysis was later performed by whole exome sequencing (WES) and Sanger sequencing (Supplementary Material 1 in the online-only Data Supplement). Two variants were detected in intron 3 and exon 8 of CYP3A5 (c.219-237A>G) and ANKK1 (c. 2137G>A), respectively.
The Naranjo algorithm was applied to assess the causal relationship between drugs and adverse events, and our case had a score of six, which indicated a “probable” relationship between domperidone and tremor (Supplementary Table 1 in the onlineonly Data Supplement). In addition, based on WHO Uppsala Monitoring Centre criteria, this movement disorder had a “certain” relationship with domperidone. In a literature search, domperidone-induced CNS side effects were only observed in infants or young children because of their poorly developed BBB and in older individuals with increased BBB permeability thought to be due to dementia. To the best of our knowledge, the woman in current study, who had no underlying disease and an intact BBB, is the first case in this age group to be reported to have acute adverse reactions. Although several cases exhibiting domperidone-induced extrapyramidal symptoms have been described, the causal factors remain elusive. In 1991, it was suggested that the dystonic reaction was induced by domperidone in young women (16 and 28 years old) with polycystic ovary syndrome due to chronic estrogenic stimulation [2]. However, the woman in current study had a normal medical history; thus, the possibility that estrogen levels affected lingual tremor could be ruled out.
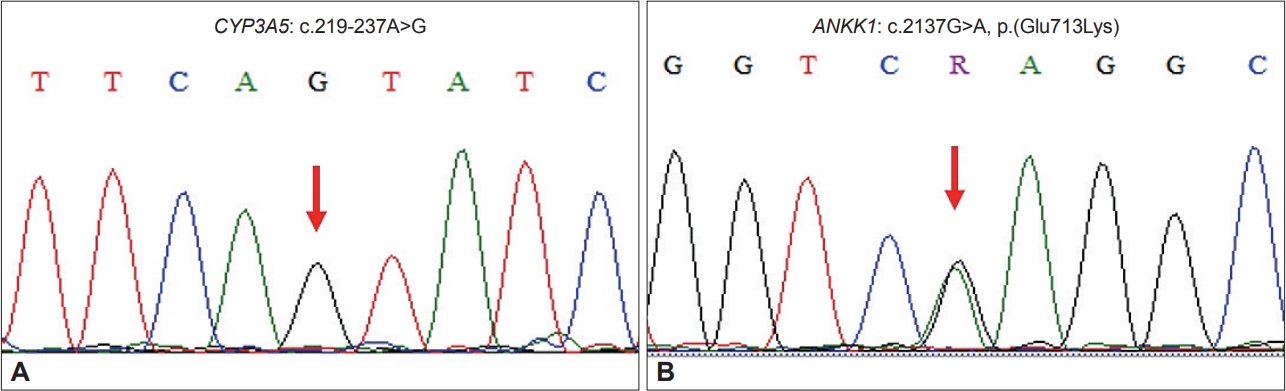
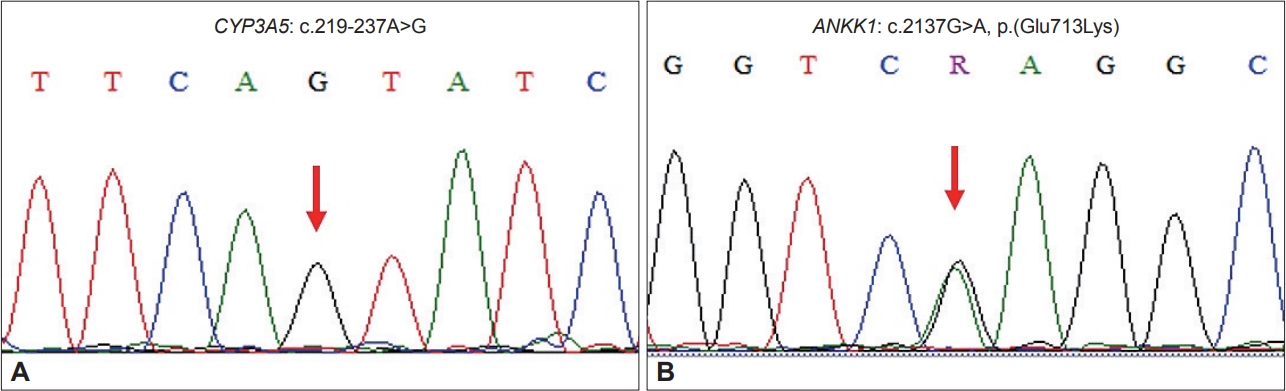
In the present work, from a pharmacogenetics perspective, we investigated the accelerating factors provoking involuntary tongue tremor after domperidone intake. As a result, WES did not reveal any clinically significant variants of CYP3A4, ABCB1, or DR2D genes encoding proteins responsible for domperidone metabolism in the liver, domperidone transporters at the BBB or domperidone targets at the striatum, respectively (Supplementary Table 2 in the online-only Data Supplement). Noticeably, a CYP3A5 homozygous variant in intron 3 (NM_000777.5:c.219-237A>G, designated CYP3A5*3) was detected by Sanger sequencing (Figure 1A). In the liver, domperidone is mainly metabolized by CYP3A4/5, producing hydroxylated metabolites. The patient carrying the homozygous genotype CYP3A5*3/*3 could not produce active enzyme. Even though no defective allele of CYP3A4 was detected, the contribution of CYP3A5 enzyme deficiency to plasma accumulation of domperidone could not be excluded.
In contrast to other dopamine antagonists, including antipsychotics (haloperidol) and antiemetics (metoclopramide), domperidone is normally extruded by the efflux transporter ABCB1 expressed on endothelial cells of the BBB, which explains the minimal central effects of this drug. In our patient, the CNS effect began soon after the first dose, demonstrating that the brain penetrance of domperidone was increased. However, no genetic variant affecting ABCB1 transporter function was detected in the patient. Notably, the patient was also prescribed esomeprazole, a proton pump inhibitor, which was listed in DrugBank as an ABCB1 inhibitor (go.drugbank.com) and approved by the FDA for ABCB1 inhibition activity [3]. Previous animal studies showed increased brain permeability of domperidone when mdr1 was deleted [4] and following treatment with an ABCB1 inhibitor [5]. At present, although evidence regarding esomeprazoleinduced domperidone aggregation in the CNS has not yet been documented, medical doctors still should be aware of extrapyramidal reactions triggered when patients are coadministered these two drugs. WES also resulted in a heterozygous variant of ANKK1 (NM178510.1:c.2137G>A, p.[Glu713Lys]) (Figure 1B), which was associated with a 40% reduction in D2 receptor expression in the striatum without affinity alteration [6]. Mechanistically, it has been hypothesized that drug-induced movement disorder results from an imbalance in the dopaminergic-cholinergic signaling system in the basal ganglia. In our patient, onset of tremor occurred within 2–3 hours after the first dose and became well defined following the second dose. As previously reviewed, the higher the blocked D2 receptor percentage, the greater the risk of acute dystonia [7]. Due to the reduced density of striatal receptor D2 in the patient, we postulate that she could have been more sensitive to dopamine signaling inhibition via D2 receptor blockade despite using the lowest recommended dose (10 mg, twice per day). Although the pathogenesis of extrapyramidal symptoms cannot be defined solely by this case, both genetics and coadministered drugs still deserve consideration, especially in individuals with an intact BBB. Furthermore, extended clinical observations are critical to investigate whether esomeprazole and genetic susceptibility predispose patients to CNS side effects or these symptoms were coincidental events.
Our study highlights the risk of extrapyramidal side effects when prescribing domperidone with esomeprazole or any ABCB1 inhibitors as concomitant therapy. In addition, genetic screening for pharmacogenes encoding drug metabolism enzymes, drug transporters and drug targets might be beneficial in cautious use of this drug.
This video shows abnormal involuntary movement of the patient’s tongue and mouth after administering a dose of 20 mg domperidone. She had no control over her tongue. This is a sign of induced extrapyramidal symptoms.
Notes
Ethics Statement
All procedures in this study were performed in accordance with ethical standards by ethics committees of the Institute of Genome Research, Vietnam Academy of Science and Technology (approval no. 3-2019/NCHGHĐĐĐ). Written informed consent was received from the patient to publish this report and any accompanying images/videos.
Conflicts of Interest
The authors have no financial conflicts of interest.
Funding Statement
This work was partially supported by the Ministry of Science and Technology of Vietnam (Grant No: KC10.40/16-20).
Author Contributions
Conceptualization: Nguyen Dang Ton, Nguyen Duc Thuan. Data curation: Vu Phuong Nhung, Hoang Thi Dung, Nhu Dinh Son, Nguyen Hai Ha. Investigation: Vu Phuong Nhung, Hoang Thi Dung, Nhu Dinh Son, Nguyen Hai Ha. Supervision: Nguyen Dang Ton, Nguyen Duc Thuan. Writing—original draft: Nguyen Duc Thuan, Vu Phuong Nhung. Writing—review & editing: all authors.
Acknowledgments
We deeply appreciate the patient for her agreement to participate in this study.
Figure 1.
Sequencing analysis showed variants in the CYP3A5 and ANKK1 genes. A: Partial sequence of CYP3A5 with a homozygous substitution in intron 3 (c.219-237A>G). B: Partial sequence of ANKK1 with a heterozygous variant in exon 8 (c.2137G>A), leading to amino acid replacement p.(Glu713Lys). Mutated nucleotides are denoted by red arrows.
REFERENCES
1. Barone JA. Domperidone: a peripherally acting dopamine2-receptor antagonist. Ann Pharmacother 1999;33:429–440.ArticlePubMedPDF
2. Bonuccelli U, Nocchiero A, Napolitano A, Paoletti AM, Melis GB, Corsini GU, et al. Domperidone-induced acute dystonia and polycystic ovary syndrome. Mov Disord 1991;6:79–81.ArticlePubMed
3. Lai JI, Tseng YJ, Chen MH, Huang CF, Chang PM. Clinical perspective of FDA approved drugs with P-glycoprotein inhibition activities for potential cancer therapeutics. Front Oncol 2020;10:561936.ArticlePubMedPMC
4. Schinkel AH, Wagenaar E, Mol CA, van Deemter L. P-glycoprotein in the blood-brain barrier of mice influences the brain penetration and pharmacological activity of many drugs. J Clin Invest 1996;97:2517–2524.ArticlePubMedPMC
5. Dan Y, Murakami H, Koyabu N, Ohtani H, Sawada Y. Distribution of domperidone into the rat brain is increased by brain ischaemia or treatment with the P-glycoprotein inhibitor verapamil. J Pharm Pharmacol 2002;54:729–733.ArticlePubMedPDF
6. Pohjalainen T, Rinne JO, Någren K, Lehikoinen P, Anttila K, Syvälahti EK, et al. The A1 allele of the human D2 dopamine receptor gene predicts low D2 receptor availability in healthy volunteers. Mol Psychiatry 1998;3:256–260.ArticlePubMedPDF
7. van Harten PN, Hoek HW, Kahn RS. Acute dystonia induced by drug treatment. BMJ 1999;319:623–626.ArticlePubMedPMC
Figure & Data
References
Citations
Citations to this article as recorded by
No Measurable Transfer of Oxytocin-Receptor Agonist Merotocin Detected in Human Breast Milk Teresa Baker, Ulrike Lorch, Yu Bagger, Carina Holmqvist, Daniël M. Jonker, Lorien E. Urban, Thomas W. Hale Breastfeeding Medicine.2024;[Epub] CrossRef
Drugs in Focus: Domperidone Maria Giovanna Puoti, Amit Assa, Marc Benninga, Ilse Julia Broekaert, Francisco Javier Martin Carpi, Marco Deganello Saccomani, Jernej Dolinsek, Matjaz Homan, Emmanuel Mas, Erasmo Miele, Christos Tzivinikos, Mike Thomson, Osvaldo Borrelli Journal of Pediatric Gastroenterology & Nutrition.2023; 77(2): e13. CrossRef
 E-submission
E-submission
 , Vu Phuong Nhung2*
, Vu Phuong Nhung2*
 PubReader
PubReader ePub Link
ePub Link Cite
Cite