The Four Square Step Test for Assessing Cognitively Demanding Dynamic Balance in Parkinson’s Disease Patients
Article information

Abstract
Objective
The Four Square Step Test (FSST) is a tool that assesses dynamic balance during obstacle step-over. To date, few studies have used the FSST to measure balance in patients with Parkinson’s disease (PD). This study aimed to verify that patients with PD, even at the de novo early stage, take more time to perform the FSST and identify which factors, cognitive status or cardinal motor symptoms, are related most to FSST scores.
Methods
Thirty-five newly diagnosed drug-naïve patients with PD and 17 controls completed the FSST. The Unified Parkinson’s Disease Rating Scale (UPDRS), Hoehn and Yahr (H&Y) stage, spatiotemporal gait parameters, and neuropsychological test battery were also assessed in the PD group.
Results
Mean FSST performance time was 8.20 ± 1.61 seconds in patients with PD, which was significantly more than the control group (7.13 ± 1.10 seconds, p = 0.018). UPDRS part III total score and H&Y stage were not significantly associated with FSST, but among the UPDRS subscores, only the postural instability/gait disturbance subscore showed a significant association. Regarding the association between FSST and cognition, the Trail Making Test-B and the Color Word Stroop Test showed strongly inverse correlations with FSST (rho = -0.598 and -0.590, respectively). With respect to gait parameters, double support time was significantly associated with FSST score (rho = 0.342, p = 0.044); however, other parameters, including velocity and step length, were not associated with the FSST.
Conclusion
The FSST can be used in the clinic to assess dynamic balance with cognitive demands even in the early stages of PD.
Parkinson’s disease (PD) has been established as a disease with cardinal motor symptoms, including bradykinesia, rigidity, and resting tremor [1]. Furthermore, gait and balance impairment are two of the most disabling PD symptoms that can also manifest in the early stage of the disease.
Cognitive impairments in PD have been linked to motor disability and especially to postural instability and gait disturbances [2]. Clinical rating scales derived from the Unified Parkinson’s Disease Rating Scale (UPDRS) and its postural instability/gait disturbance (PIGD) subscore have been used to examine the relationship between cognitive and motor impairment [3]. According to previous studies, dynamic balance problems in PD are contributed to by simple postural instability and cognitive impairment [4]. In this regard, a growing number of studies have investigated the influence of dual-task demands on gait and balance in patients with PD. Unfortunately, diverse methodologies and conflicting outcomes reported in previous studies make it difficult to draw conclusions [5].
The Four Square Step Test (FSST) is an easy and quick bedside exam that is available to assess dynamic balance in terms of the ability to rapidly cross over obstacles and to change direction in the clinical setting [6]. First validated in healthy older adults in 2002, many papers have been published that have used it, not only for musculoskeletal problems but also for central nervous system (CNS) diseases such as chronic stroke, multiple sclerosis, and Huntington’s disease [7-9]. Unlike previous instruments for measuring dynamic balance in PD, such as tandem gait, the Timed Up and Go and the mini-Balance Evaluation Systems Test (BESTest), the FSST is a more cognitively demanding locomotor task that involves complex cognitive-motor control by requiring participants to remember and complete a series of steps. Given the strong relationship between dynamic balance and cognition, we thought the FSST could be a more appropriate measurement instrument to assess dynamic balance in patients with PD.
To date, there have been only two reports on FSST used in patients with PD. In these studies, the FSST test showed good interrater reliability, and the FSST performance time was longer in patients with PD than in age-matched controls [10]. Additionally, a previous study showed that the FSST was associated with executive function as evaluated by the Trail Making Test B (TMT-B) in patients with PD [11]. However, these studies were conducted only in patients with PD who had been diagnosed several years prior and who took dopaminergic drugs. Therefore, we aimed to test whether impaired FSST performance is also observed in early-stage, drug-naïve PD patients, and if so, which motor, cognitive, and gait measures were related to FSST performance.
MATERIALS & METHODS
Participants
Thirty-five patients with de novo PD, as defined by standard criteria [12], were recruited from the Parkinson’s Disease Center, Korea University Guro Hospital from July 2018 to February 2019. The diagnosis of PD was confirmed by movement disorder specialists in our center and was also supported by dopamine transporter positron emission tomography (18F-FP-CIT PET).
We only included drug-naïve de novo patients in the early disease stage who were below Hoehn and Yahr (H&Y) stage 3 (could walk without any devices or assistants) and had never been treated with dopaminergic drugs. Patients were excluded if they had dementia, definite autonomic dysfunction, downward saccadic slowness (including ”Round the houses sign”) or other red flag signs suggesting atypical parkinsonism. Patients who had a history of previous falls or performed poorly on the pull test (2 or greater score on the UPDRS part III-30) were excluded because of safety risks and the possibility they had atypical parkinsonism. Patients were also excluded if they had a history of stroke, head trauma, or other neurological and musculoskeletal diseases that could likely contribute to gait disturbances.
The patients with PD were compared with 17 control subjects who were diagnosed with essential tremor and did not have parkinsonism. Additionally, this control grouponsisted of only those who had no gait and balance dysfunction during an examination and no comorbidity that could affect gait and balance. All information from the PD patients and controls was collected retrospectively. The Institutional Review Board at Korea University Guro Hospital approved the study, and participants signed written informed consent forms before participating.
Procedures and measurements
The FSST requires participants to step over small and low obstacles (horizontal and vertical length of the obstacle 90 cm, height of the obstacle 2.5 cm, side length of the outer box border 1 m) placed in a cross configuration by generally following the initial protocol used in a previous study [6]. At the start of the test, the participants stand on the first (lower left) square with both feet close together and are instructed to take one step at a time over each obstacle in a clockwise direction as rapidly and as safely as possible, touching each square with both feet before moving to the next square: first moving forward, then to the right, backwards, then left to their original position. Then, they should immediately repeat the same steps in the counterclockwise direction (Figure 1). After one practice trial, the patient time was recorded for the next two trials, and the best time in seconds was used as the FSST score. The assessor was blinded to the participant’s group.

Setup of the Four Square Step Test (FSST) in our laboratory. The subject should be ready in quadrant 1. When the examiner says, “Go,” the subject starts stepping clockwise through quadrants 2 → 3 → 4 → 1, and when he/she reaches quadrant 1 again, they go back counterclockwise through quadrants 4 → 3 → 2 → 1. Subjects should take one step at a time over each obstacle as rapidly and safely as possible, touching each square with both feet before moving to the next square.
UPDRS part III and H&Y stage were administered and scored by one trained rater and confirmed by three movement disorder specialists via recorded video review. The bradykinesia subscore of the UPDRS-III was calculated by summing the scores for items 15–22 and 27, and the PIGD subscore was obtained by summing items 23–26. We also assessed spatiotemporal gait parameters (i.e., gait velocity, cadence, step length, base, percentage of double and single support, and percentage of swing and stance phase during walking at a comfortable speed) using the computerized GaitRite System (CIR Systems, Inc., Franklin, NJ, USA). The Korean version of the Montreal Cognitive Assessment (K-MoCA) was administered to all patients with PD, and we also used the percentile score adjusted by age, sex and education age for each cognition test in the Seoul Neuropsychological Screening Battery (SNSB), including the Digit-Span Test (DST), the Korean version of the Boston Naming Test (K-BNT), the Rey Complex Figure Test (RCFT), the Seoul Verbal Learning Test (SVLT), the Digit Symbol Coding (DSC), the Controlled Oral Word Association Test (COWAT), the TMT-B and the Color Word Stroop Test (CWST), if it was administered.
Statistical analysis
Descriptive statistics were calculated for age, sex, disease duration, and education. Differences in FSST performance time between patients with PD and control groups were examined using t-tests (for continuous variables) and chi-squared or Fisher’s exact tests (for nominal variables). The FSST performance times were not normally distributed; therefore, the association between the FSST and concurrent motor and cognitive measures and spatiotemporal gait parameters were determined with Spearman’s correlation coefficient. All analyses were performed using SPSS software (IBM SPSS Statistics for Windows, version 20.0; IBM Corp., Armonk, NY, USA). All reported p values were 2-tailed. The level of significance was set at p < 0.05.
RESULTS
Thirty-five patients with PD and seventeen controls participated in this study. The clinical characteristics of all participants are reported in Table 1. No falls or injuries occurred during the testing. There were no significant differences in age or sex ratio between the PD and control groups. In the PD group, the mean disease duration, which was calculated using the year of symptom onset, was 14.14 months, and the mean UPDRS part III total score was 23.8. The mean FSST performance time was 8.20 ± 1.61 seconds in the PD group, which was significantly different from that in the control group (7.13 ± 1.10 seconds, p = 0.018). The FSST performance time was significantly correlated with age (rho = 0.531, p = 0.001) and disease duration (rho = 0.356, p = 0.036) only in the PD group (Table 2).
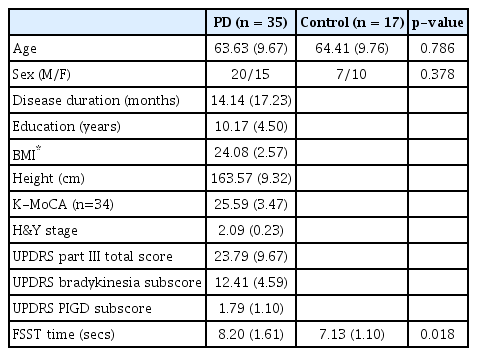
Clinical characteristics

Correlation between the FSST performance time and other clinical elements
In terms of motor symptoms and disease severity, the UPDRS part III total score and H&Y stage were not significantly associated with the FSST performance time. However, among the UPDRS subscores, the PIGD subscore showed a significant FSST performance association, but the bradykinesia subscore did not (Table 2). Next, we intended to elucidate the association between the FSST and cognition, but the K-MoCA score was not associated with FSST performance. After analyzing the results of the SNSB of 18 PD patients whose data for the full cognition test battery were available (Supplementary Table 1 in the online-only Data Supplement), we found there was no significant correlation between the FSST and all cognitive domains, including attention, language, memory, visuospatial, and frontal/executive function. However, an analysis of each individual test showed that TMT-B and CWST were strongly and significantly inversely correlated with FSST performance (worse TMT-B or CWST scores were associated with longer FSST performance times) (Table 3). Because in these 18 patients, disease duration was not significantly correlated with the FSST (rho = 0.258, p = 0.302) and each domain and test value was the percentile score, which already took into account the participant’s age and education level, there was no need to adjust for age and disease duration in this statistical analysis.

Correlation between the FSST performance time and cognition
Correlations between the FSST time and the spatiotemporal gait parameters are presented in Table 4. Only the percentage of double stance was significantly correlated with the FSST time, whereas velocity, cadence, step length, and the coefficient of variation of step length and base were not statistically significantly correlated with FSST time.
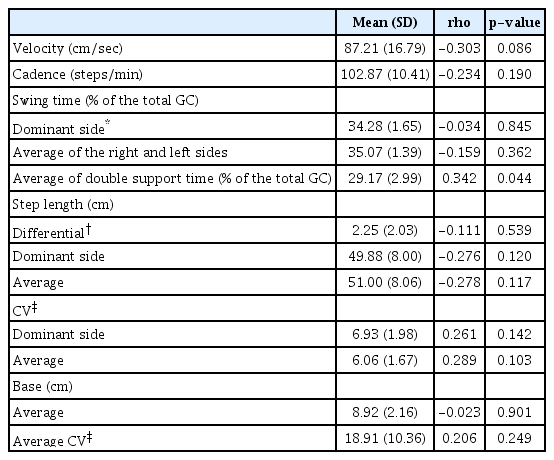
Correlation between the FSST performance time and the spatiotemporal parameters of the gait analysis
DISCUSSION
To our knowledge, this is the first study to examine whether patients with PD show differences in FSST performance even when they are drug-naïve and in the early disease stage. According to our results, patients with PD, even in the early disease stage, showed slower FSST performance times than the control group. The mean performance time measured in this study was slightly faster than that in previous studies (8.20 sec in ours vs. 9.52 sec in [10] and 12.9 sec in [11]), which may be due to the early disease stage and short disease duration in our participants. The FSST has been used as a balance test to anticipate falling tendency in healthy older adults, and among those with vestibular disorders, musculoskeletal conditions such as joint replacement and osteoporosis, and CNS disorders such as stroke, multiple sclerosis and Huntington’s disease [13].
There are two studies so far that have used the FSST in patients with PD. In these studies, the reliability and validity of the FSST were established, but it was not as good as other tests (e.g., the Mini-BESTest) at distinguishing between fallers and nonfallers [10]. The FSST performance time was correlated with disease severity, as measured by both the UPDRS and H&Y stage [11]. Unlike our study, these previous studies were conducted in patients with mild to moderate PD who had already been diagnosed with PD and were taking dopaminergic drugs (mean disease duration 6.25 years, mean UPDRS part-III score 28.6), including some fallers or freezers. Our results obtained in newly diagnosed patients with early-stage PD showed that FSST performance was not associated with the severity of motor symptoms such as bradykinesia and was also not associated with spatiotemporal gait parameters (i.e., velocity, cadence, and step length in gait analysis). Instead, frontal/executive function (TMT-B and CWST) was strongly correlated with the FSST performance. Considering our results that the UPDRS PIGD subscore and double support time in gait analysis were correlated with FSST performance, the FSST acts primarily as a balance test, as it has been used so far. Therefore, we can suggest that the FSST functions as a balance test that incorporates some cognitive functionality.
There are two distinct types of balance, simple static and dynamic balance. The latter has more meaning of the ability of a person to balance while in motion or while switching between positions. Past studies have described balance impairment and falling as the two main motor problems that are observed in the advanced stages of PD, and they are accompanied by the progression of other cardinal motor symptoms. If balance impairment instruments such as the pull test and tandem gait test are abnormal in the early disease stage, this is thought to suggest atypical parkinsonism [14]. However, falling in PD is not only a simple static balance problem when standing or walking but also a dynamic balance problem when turning, obstacle-crossing, and during dual-task performance. Dynamic balance is multidimensionally affected by lower extremity muscle strength, sensory integration ability, and frontal/executive functions, as well as parkinsonian motor symptoms [15,16]. Above all, previous articles reported that executive functions, particularly those involving set shifting and inhibition, were associated with worse balance and gait performance in patients with PD [4]. Based on our studies, we proposed that even though it is not overtly obvious in patients’ daily living, impairment of dynamic balance also exists in the early stage of PD, and this dynamic imbalance in patients with early-stage PD is mainly related to frontal lobe executive dysfunction, among other factors that affect dynamic balance.
Numerous rating scales and clinical tests that have been demonstrated to be valid and reliable as dynamic balance tests for PD are already used worldwide. Among them, several, such as the Tinetti Balance Scale, Berg Balance Test, and the mini-BESTest, are recommended or suggested by the Movement Disorder Society [17]. However, these tests cannot evaluate the cognitive components of dynamic balance that require executive function. Furthermore, while the FSST score is analyzed as a continuous variable that measures performance time in seconds, the results from the other scales or tests mentioned above show strong ceiling or floor effects [17]. In this regard, the FSST can be a useful assessment that compensates for the limitations of traditional instruments and adds the ability to evaluate dynamic balance in patients with PD.
It is an interesting and instructive finding that FSST performance was not significantly associated with other tests of frontal/executive function (i.e., MoCA, DSC, and the COWAT) but was strongly correlated with the TMT-B and CWST. Unlike the former, the latter is more similar to the FSST process in that the latter is more visuocognitively demanding. In addition to simple visual abilities such as visual acuity, visuocognition, which requires an interaction between visual and cognitive function, is also important for gait stability and adaptability [18]. Vision and cognition have been found to be separately related to gait impairment, but the interactive effect of both has not been investigated. Knowledge of visuocognitive processes during gait is essential and important to fully understand the mechanisms underlying gait and balance impairment in patients with PD. Therefore, measurement instruments that can also reveal visuocognitive effects on gait and balance are indispensable. For this reason, a few investigators have reported using their own instruments or assessments that can explain more complex walking adaptability in the context of visuocognitive processing [19], but they are still not very feasible and have not been standardized and validated. We suggest that the FSST could be a good candidate instrument, as it is an easily administered, comprehensive gait and balance scale that assesses all relevant constructs, including executive functions and visuocognitive interactions.
This study has several limitations. First, some information for the control group, such as education, BMI, cognitive tests, and gait parameters, was not available. This makes it challenging to determine whether worse FSST performance in the PD group than in the control group was due to worse cognitive function. Next, our sample size was somewhat small, and fully available data were limited. However, since we introduced the FSST as an easy and feasible test in this study, we planned a future study with a larger sample size that will be conducted soon. Last and the most important limitation is that we used essential tremor patients as a control group. As already mentioned in many studies, essential tremor has many features associated with gait, balance and cognition. Although we only included people who showed only an action tremor without any gait or balance problems in the examination, we admit that this could be an inevitable limitation of this research.
Conclusion
In this study, we found that FSST performance was impaired even in de novo, early-stage patients with PD, and this was associated with executive function. The FSST is a feasible measurement for balance in the clinical field (quick to administer, objectively scored in seconds, requires little space and cost). Not only is it suitable for assessing dynamic balance, but it is also unique in that it requires executive function and visuocognitive processing. Therefore, administration of the FSST helps assess motor-cognitive interactions in PD and it is especially useful for investigating associations between dynamic balance and executive function.
Supplementary Materials
The online-only Data Supplement is available with this article at https://doi.org/10.14802/jmd.20146.
Percentile score of each domain and each test of neuropsychiatric battery
Notes
Conflicts of Interest
The authors have no financial conflicts of interest.
Author Contributions
Conceptualization: Jinhee Kim, Seong-Beom Koh. Data curation: Jinhee Kim, Ilsoo Kim, Ye Eun Kim. Formal analysis: Jinhee Kim. Investigation: Jinhee Kim, Ilsoo Kim, Ye Eun Kim. Methodology: Jinhee Kim, Ilsoo Kim, Seong-Beom Koh. Project administration: Seong-Beom Koh. Resources: all authors. Software: Jinhee Kim. Supervision: Seong-Beom Koh. Validation: Ilsoo Kim, Ye Eun Kim. Visualization: Jinhee Kim. Writing—original draft: Jinhee Kim. Writing—review & editing: all authors.
Acknowledgements
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.