COVID-19 Associated Acute Necrotizing Encephalopathy Presenting as Parkinsonism and Myorhythmia
Article information

Dear Editor,
Coronavirus disease 2019 (COVID-19)-associated acute necrotizing encephalopathy (ANEC) has rarely been reported with unknown true prevalence. It has severe neurological consequences with high mortality if it is not detected [1]. Herein, we describe a suspected case of COVID-19-associated ANEC with presenting features of parkinsonism and myorhythmia. We were given written informed consent to disclose the information reported in this letter.
A previously healthy 31-year-old man presented with a nine-day history of fever, cough, and worsening shortness of breath. His chest radiograph showed bilateral ground-glass opacities, and he tested positive for COVID-19 by reverse-transcriptase polymerase chain reaction (PCR) from nasal swabs. He required nasal cannula supplemental oxygen and was given 8 mg intravenous dexamethasone daily, 1,800 mg favipiravir tablets twice daily and subcutaneous low-molecular-weight heparin. His condition worsened with agitation, restlessness, and fluctuating consciousness. On the second day of admission, he was prescribed 5 mg haloperidol tablets bid for one day, tapered to 3 mg bid for two days and 1.5 mg bid for another two days to manage his restless behavior. He was referred to the neurology team for assessment on day six of admission.
Upon review, he was disorientated but able to follow simple commands. He had involuntary jaw opening with slow rhythmic movements of his lower facial muscles at rest, which also interfered with his speech (Supplementary Video 1, Part 1 in the online-only Data Supplement). There were no abnormal palatal or lingual movements. He had reduced eye blinking, hypometric horizontal saccade and jerky pursuit. He was able to pantomime but had micrographia, mild bilateral upper limb rigidity, slow finger tapping and absence of arm swing while walking. His brain MRI demonstrated bilateral symmetrical T2/fluid attenuated inversion recovery thalamic hyperintensities with hemosiderin deposition and patchy contrast enhancement. Subtle hyperintensities were present in the pons. Time-of-flight MR venography and angiography were normal with no arterial or venous thrombosis (Figure 1). His blood parameters showed lymphopenia, thrombocytopenia, raised C-reactive protein (12.2 mg/L, 0–11 mg/L), D-dimer (1,652 ng/mL, 0–246 ng/mL) and serum ferritin (4,256 μg/L, 22–322 ng/mL). His cerebrospinal fluid was acellular with a protein level of 0.65 g/L (0.08–0.32 g/L) and a glucose level of 5.6 mmol/L (2.2–3.9 mmol/L); cultures and SARS-COV-2 PCR were negative. Serum autoimmune encephalitis (anti-AMPA 1/2, anti-CASPR2, anti-LGI1, anti-DPPX, anti-GABA-B, and anti-NMDAR) and paraneoplastic antibody screening (anti-amphiphysin, anti-CV2 antigen, anti-PNMa2ab, anti-Ri, anti-Yo, anti-Hu, anti-recovery, anti-SOX1, and anti-titin) were negative. His electroencephalogram showed features of encephalopathy with diffuse slowing in the theta range.
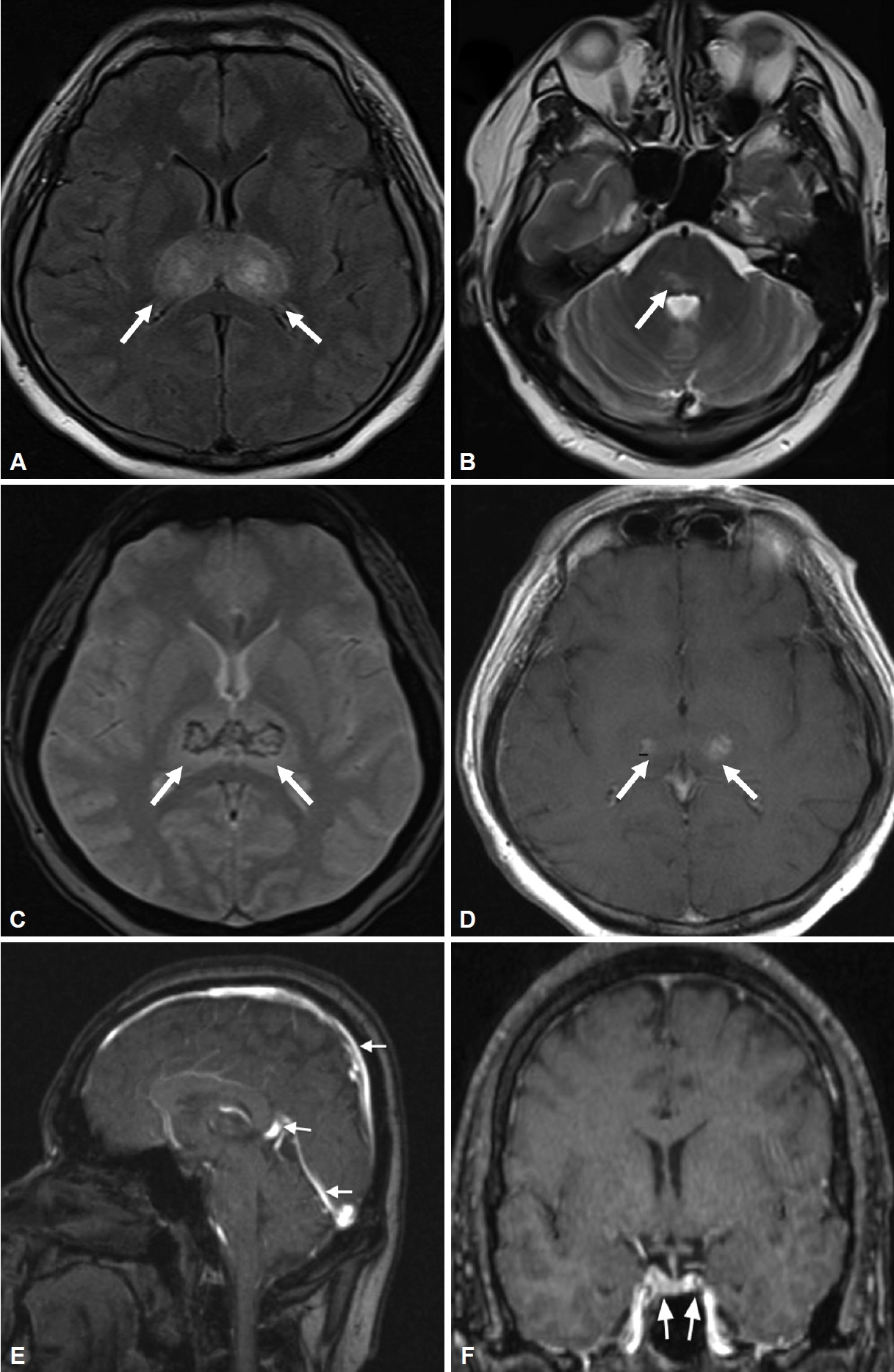
Cranial magnetic resonance imaging of the patient obtained on day 17 of illness. A and B: Axial FLAIR and T2W MRI images demonstrate diffuse hyperintense lesions bilaterally symmetrical within the deep gray matter of the bilateral thalami and right posterior pons (arrows). C: Axial T2W GRE revealed susceptible artifacts within thalamic lesions with hemosiderin deposits (arrows). D: The thalamic lesions showed subtle enhancement on T1W postcontrast (arrows). E: Sagittal venogram TOF showed no filling defect within the superior sagittal sinus, great cerebral vein or straight sinus (arrows). F: Coronal venogram at the level of the cavernous sinuses showed no filling defect within the cavernous sinuses (arrows). FLAIR, fluid attenuated inversion recovery; GRE, gradient echo; TOF, time of flight.
A diagnosis of ANEC was made, and he was given intravenous methylprednisolone at a dose of 1 g daily for three days and trihexyphenidyl 2 mg tds. Three days after completing methylprednisolone, he showed significant cognitive improvement with resolution of the abnormal movements (Supplementary Video 1, Part 2 in the online-only Data Supplement).
Our case is interesting due to the concomitant presentation of abnormal movement disorders in a rare occurrence of COVID-19-associated ANEC. ANEC is more frequently encountered in children than adults and is characterized by multiple, symmetrical lesions in the thalami, striatum, and brainstem. ANEC is a parainfectious neurological complication of COVID-19 infection due to a hyperimmune response with coma, and encephalopathy dominates the clinical presentation with limited outcome data (Supplementary Table 1 in the online-only Data Supplement).
Abnormal movement disorders in COVID-19-associated ANEC have not been reported. Our patient presented with involuntary jaw opening and rhythmic slow movements of the lower facial muscles involving the lower orbicularis oris, mentalis and depressor muscles, consistent with the phenomenology of myorhythmia. Myorhythmia is characterized by 1–4 Hz movement typically involving the cranial and limb muscles of possible subcorticalsupraspinal origin [2]. Myorhythmia is usually associated with lesions in the brainstem, thalamus, and other diencephalic structures with potentially treatable conditions, as in our case of ANEC [2]. Other potential etiologies are thalamic and brainstem infarcts, Whipple’s disease, autoimmune encephalitis and drug intoxication [2]. Overall cerebrovascular damage is the most common cause, and isolated facial myorhythmia involving the lips and other lower facial muscles has been reported in thalamic infarcts [3]. Myorhythmia can also occur alongside other movement disorders, such as dystonia and parkinsonism, due to disrupted basal gangliathalamo-frontal cortical circuits [2]. Unlike the previously reported cases, the facial myorhythmia observed in our patient was more prominent at rest and did not affect his swallowing ability [3,4].
There have also been reported cases of myorhythmia and rhythmic jaw opening in large brainstem hemorrhage and lesions involving the pontine tegmentum and pontine reticular formation [2]. Our patient had lesions in the thalamus and pons, which could explain the parkinsonism and myorhythmia that may have manifested as involuntary jaw opening. Treatment with neuroleptics can interfere with the clinical picture, as we were uncertain of the time of onset of these abnormal movements. However, drug-induced myorhythmia is rare and has only been reported as a side effect of interferon alpha-2a therapy and phenytoin [5,6]. Although haloperidol may cause parkinsonism, it is important to consider potentially treatable parainfectious neurological sequelae as a differential diagnosis. We hypothesize that the rapid and dramatic temporal improvement of parkinsonism and myorhythmia three days after intravenous methylprednisolone supports the notion that the abnormal movements may have originated from a single entity of virus-induced neuroimmunopathology in ANEC rather than manifesting as side effects of haloperidol. As such, the short course and low dose of trihexyphenidyl may have been minor contributors to his recovery.
The exact pathogenesis of ANEC is not entirely clear, but systemic inflammatory insult and hypercytokinemia have been postulated to trigger necrotic brain lesions in patients with ANEC [7]. We have no electromyographic evidence to support our findings; nevertheless, recognizing this phenomenology is crucial to assist in early clinical diagnosis and treatment to improve patient outcomes.
Supplementary Materials
The online-only Data Supplement is available with this article at https://doi.org/10.14802/jmd.21063.
Video 1.
Before treatment, the patient had slurred speech and involuntary jaw opening with myorhythmic movement of the lower facial muscles. He had bilateral bradykinesia on finger and toe tapping. His gait was slow with no arm swing. Three days following intravenous methylprednisolone at a dose of 1 gm daily for three days, he showed marked improvement with resolution of parkinsonism and myorhythmia symptoms.
Supplementary Table 1.
Summary of COVID-19 associated acute necrotizing encephalopathy reported in the literature
Notes
Ethics Statement
Written and verbal consent for publication was obtained from the patient.
Conflicts of Interest
The authors have no financial conflicts of interest.
Funding
None.
Author Contributions
Conceptualization: Tien Lee Ong, Khariah Mat Nor. Data curation: Tien Lee Ong, Khariah Mat Nor. Formal analysis: Tien Lee Ong, Khariah Mat Nor. Writing—original draft: Tien Lee Ong. Writing—review & editing: all authors.
Acknowledgements
We would like to thank the Director General of Health Malaysia for Datuk Dr Noor Hisham Abdullah permission to publish this article.