E-submission
E-submission
Articles
- Page Path
- HOME > J Mov Disord > Volume 14(3); 2021 > Article
-
Review Article
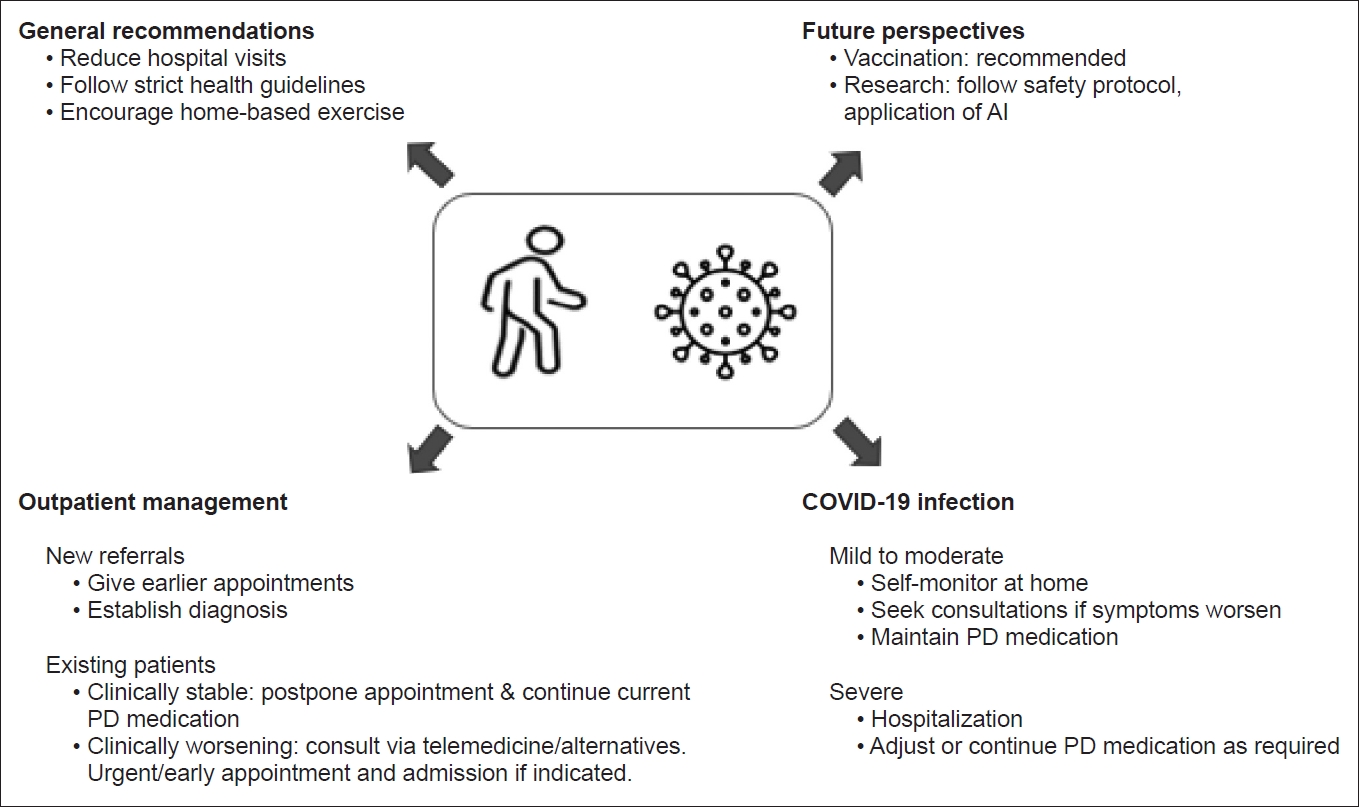
Management of Parkinson’s Disease in the COVID-19 Pandemic and Future Perspectives in the Era of Vaccination -
Yue Hui Lau1
 , Keng Ming Lau2, Norlinah Mohamed Ibrahim3
, Keng Ming Lau2, Norlinah Mohamed Ibrahim3 -
Journal of Movement Disorders 2021;14(3):177-183.
DOI: https://doi.org/10.14802/jmd.21034
Published online: July 29, 2021
1Department of Neurology, Hospital Kuala Lumpur, Kuala Lumpur, Malaysia
2Department of Internal Medicine, University Malaya Medical Centre, Kuala Lumpur, Malaysia
3Division of Neurology, Department of Internal Medicine, National University of Malaysia, Kuala Lumpur, Malaysia
- Corresponding author: Yue Hui Lau, MBBS, MRCP Department of Neurology, Hospital Kuala Lumpur, 23 Jalan Pahang, Wilayah Persekutuan Kuala Lumpur, Kuala Lumpur 50586, Malaysia / Tel: +60165003600 / Fax: +60-3-26911186 / E-mail: andrealau38@gmail.com
• Received: March 14, 2021 • Revised: April 11, 2021 • Accepted: April 22, 2021
Copyright © 2021 The Korean Movement Disorder Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
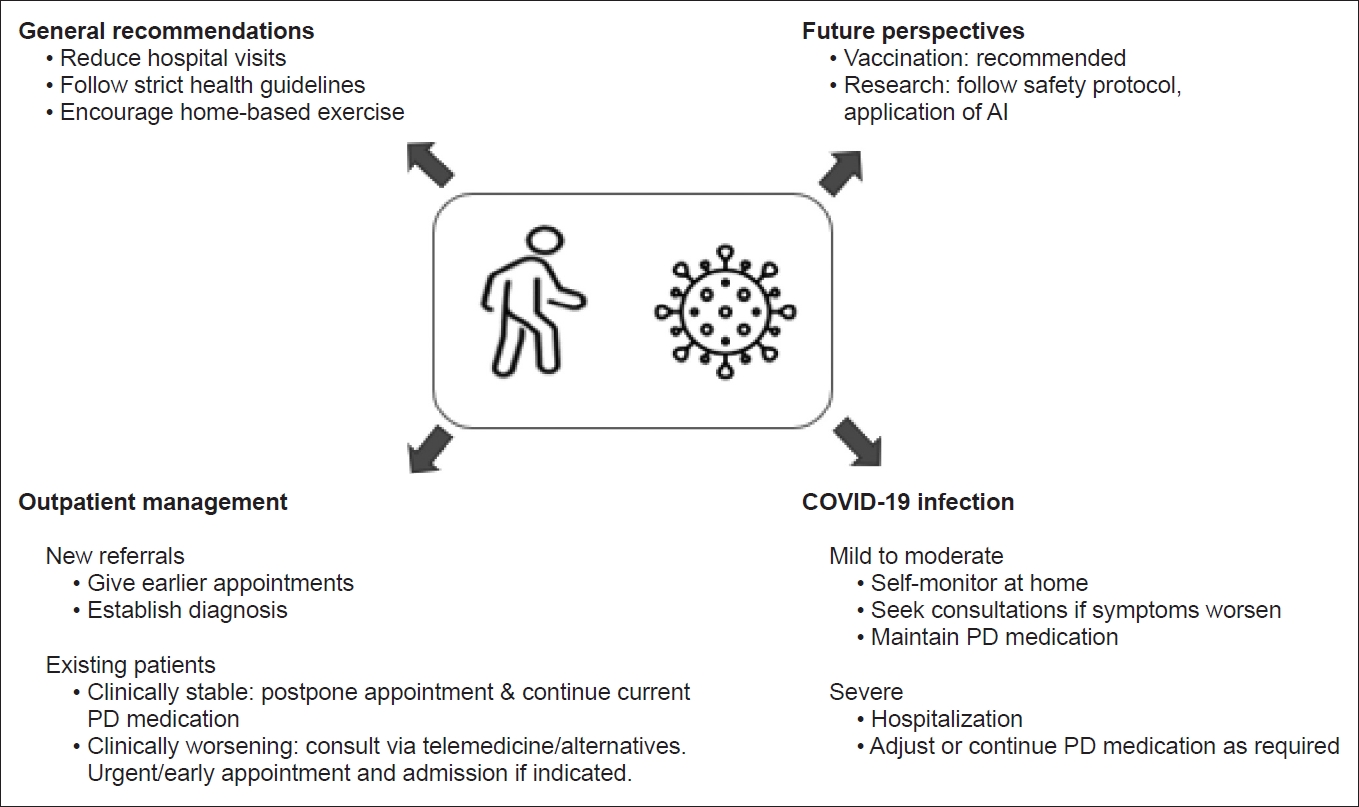
Figure & Data
References
Citations
Citations to this article as recorded by 
- Increasing exercise with a mobile app in people with Parkinson’s disease: a pilot study
Jong Hyeon Ahn, Dongrul Shin, Dongyeong Lee, Hye Young Kim, Jinyoung Youn, Jin Whan Cho, Suzanne Kuys
Brain Impairment.2024;[Epub] CrossRef - Potential convergence of olfactory dysfunction in Parkinson’s disease and COVID-19: The role of neuroinflammation
Hui Li, Junliang Qian, Youcui Wang, Juan Wang, Xiaoqing Mi, Le Qu, Ning Song, Junxia Xie
Ageing Research Reviews.2024; 97: 102288. CrossRef - A large survey on COVID-19 vaccination in patients with Parkinson’s disease and healthy population
Chao Han, Zhen Zhen Zhao, Piu Chan, Fang Li, Chun Ling Chi, Xin Zhang, Yan Zhao, Jing Chen, Jing Hong Ma
Vaccine.2023; 41(43): 6483. CrossRef - Role of SARS-CoV-2 in Modifying Neurodegenerative Processes in Parkinson’s Disease: A Narrative Review
Jeremy M. Morowitz, Kaylyn B. Pogson, Daniel A. Roque, Frank C. Church
Brain Sciences.2022; 12(5): 536. CrossRef - Deep Learning Paradigm for Cardiovascular Disease/Stroke Risk Stratification in Parkinson’s Disease Affected by COVID-19: A Narrative Review
Jasjit S. Suri, Mahesh A. Maindarkar, Sudip Paul, Puneet Ahluwalia, Mrinalini Bhagawati, Luca Saba, Gavino Faa, Sanjay Saxena, Inder M. Singh, Paramjit S. Chadha, Monika Turk, Amer Johri, Narendra N. Khanna, Klaudija Viskovic, Sofia Mavrogeni, John R. Lai
Diagnostics.2022; 12(7): 1543. CrossRef - Movement disorders in COVID-19 times: impact on care in movement disorders and Parkinson disease
Sabrina Poonja, K. Ray Chaudhuri, Janis M. Miyasaki
Current Opinion in Neurology.2022; 35(4): 494. CrossRef - Viruses, parkinsonism and Parkinson’s disease: the past, present and future
Valentina Leta, Daniele Urso, Lucia Batzu, Yue Hui Lau, Donna Mathew, Iro Boura, Vanessa Raeder, Cristian Falup-Pecurariu, Daniel van Wamelen, K. Ray Chaudhuri
Journal of Neural Transmission.2022; 129(9): 1119. CrossRef
Comments on this article
 PubReader
PubReader ePub Link
ePub Link Cite
Cite