 E-submission
E-submission
Articles
- Page Path
- HOME > J Mov Disord > Volume 16(2); 2023 > Article
-
Brief communication
Sex and Gender Influence Urinary Symptoms and Management in Multiple System Atrophy -
Elke Schipani Bailey
 , Sara J. Hooshmand, Negin Badihian, Paola Sandroni, Eduardo E. Benarroch, James H. Bower, Phillip A. Low, Wolfgang Singer, Elizabeth A. Coon
, Sara J. Hooshmand, Negin Badihian, Paola Sandroni, Eduardo E. Benarroch, James H. Bower, Phillip A. Low, Wolfgang Singer, Elizabeth A. Coon
-
Journal of Movement Disorders 2023;16(2):196-201.
DOI: https://doi.org/10.14802/jmd.23016
Published online: May 24, 2023
Department of Neurology, Mayo Clinic, Rochester, MN, USA
- Corresponding author: Elizabeth A. Coon, MD Department of Neurology, Mayo Clinic, 200 First St. SW, Rochester 55905, MN, USA / Tel: +1-507-266-3544 / Fax: +1-507-538-6012 / E-mail: coon.elizabeth@mayo.edu
Copyright © 2023 The Korean Movement Disorder Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Objective
- Multiple system atrophy (MSA) is characterized by urinary dysfunction, yet the influence of sex and gender on urinary symptoms and treatment is unclear. We sought to characterize sex and gender differences in the symptomatology, evaluation, and management of urinary dysfunction in patients with MSA.
-
Methods
- Patients with MSA evaluated at our institution were reviewed and stratified by sex.
-
Results
- While the prevalence of urinary symptoms was similar in male and female patients, incontinence was more common in females. Despite this, males and females underwent postvoid residual (PVR) measurement at similar rates. While catheterization rates were similar when PVR was measured, males were more than twice as likely to be catheterized than females in the absence of PVR measurement.
-
Conclusion
- Urinary symptoms are common in MSA, but their presentation differs between males and females. The difference in catheterization rates may be driven by a gender disparity in referrals for PVR, which can guide treatment.
- Study design
- Patients with a diagnosis of probable or possible MSA [1] evaluated at our institution from January 1998–December 2012 were included. Only patients who permitted use of their clinical records for retrospective research were enrolled in our study. Neurologic and urologic provider documentation was reviewed to characterize urinary symptoms. All symptom onset was determined based on patient recollection of duration of symptoms as detailed in this documentation, and all patients completed standardized questionnaires regarding urinary incontinence, urgency and frequency. Postvoid residual (PVR) was obtained through ultrasound or catheter at the discretion of the urologic procedure team. Documentation from emergency department visits, admissions, general practitioner evaluation, consulting services, and ancillary staff was reviewed. This study was approved by the Institutional Review Board of Mayo Clinic (#12-008800) and informed consent was received for all patients.
- Statistical analysis
- Data were analyzed using R-based BlueSky Statistics software (BlueSky, Chicago, IL, USA). Categorical variables were analyzed using chi-square tests, while continuous variables were analyzed with unpaired t tests. PVR and time to catheterization data demonstrated a positively skewed distribution and were transformed on a logarithmic scale for analysis under a normal distribution. Analysis of the time to catheterization by sex was calculated using a Kaplan‒Meier time to event analysis. Statistical significance was set at p < 0.05.
MATERIALS & METHODS
- Demographics
- The cohort of patients evaluated at our institution with a diagnosis of MSA between 1998 to 2012 has been described previously and includes 356 males (52.0%) and 329 females (48.0%) (Table 1) [10]. Most patients (65.0%) had a follow-up period at their referring center of less than 90 days. There was no sex difference in age at symptom onset, years from symptom onset to diagnosis, disease duration, or MSA subtype (Table 1).
- We found that 41% of males had a diagnosis of benign prostatic hypertrophy (BPH). Prior to diagnosis, 87 males underwent procedures to address urinary symptoms, and 82 (94.3%) of these procedures were directed at suspected prostatic involvement. By 3 months, the urinary symptoms of just 22 males had improved, and 10 of these 22 (11.5% of the entire cohort who underwent procedures) had no issues beyond 3 months. The urinary symptoms of 54 males who underwent procedures failed to improve or worsened immediately, with an overall failure in 71 (81.6% of the 87 male patients who underwent a procedure).
- In contrast to males, only 49 female patients underwent procedures to address urinary symptoms (p = 0.001), many of which were directed at pelvic floor physiology. Of those who underwent procedures, symptoms failed to improve or recurred in 45 (91.8%).
- Urinary symptoms
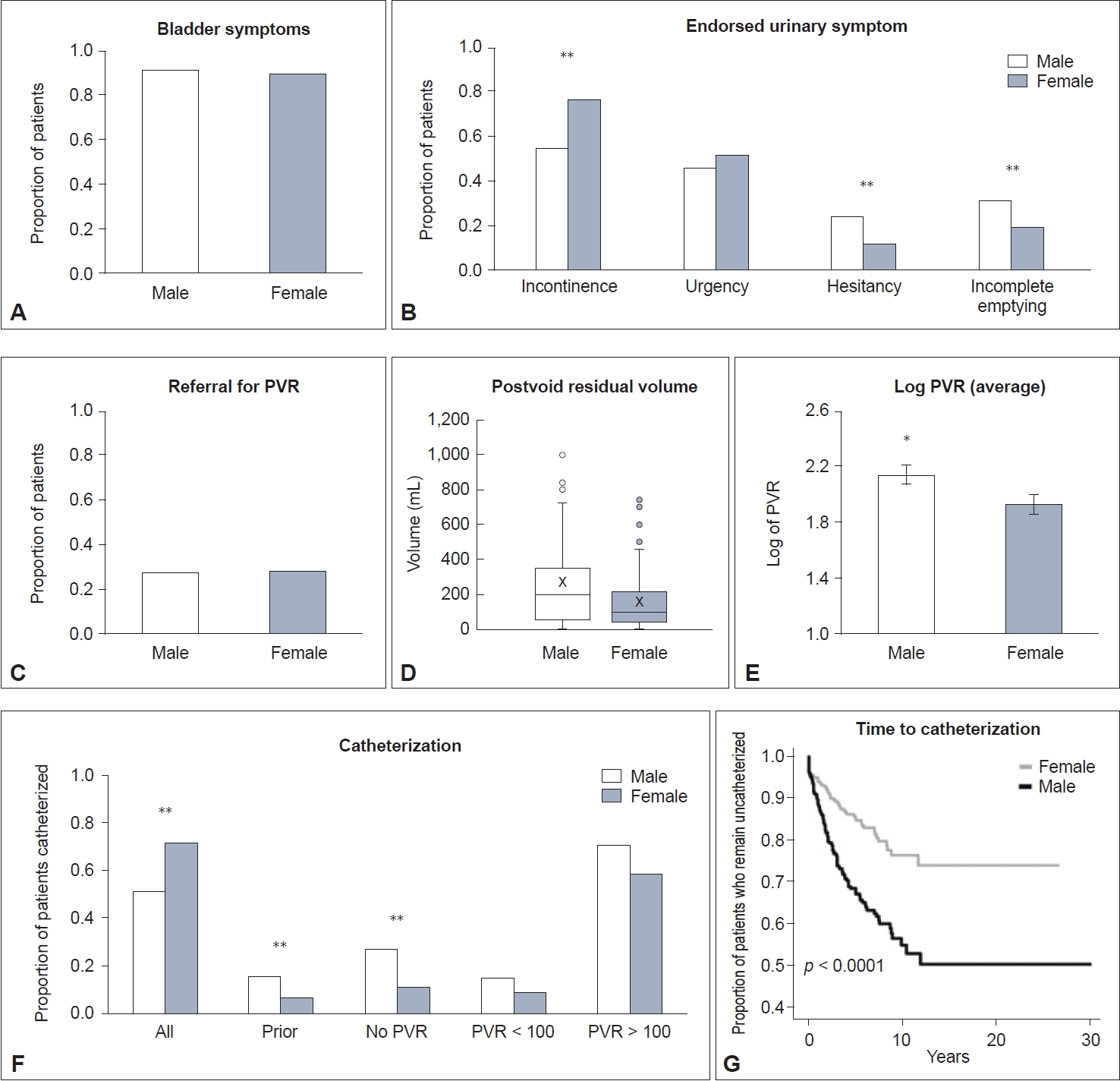
- The proportion of males and females reporting urinary symptoms in their disease course to their neurologist during an office visit was similarly high (91.9% vs. 89.1%, respectively, p = 0.212) (Figure 1A). The average time from MSA diagnosis to bladder symptom onset did not differ between males and females (1.8 vs. 2.2 ± 0.2 years, p = 0.17), and there was no sex difference in the proportion of patients who developed bladder symptoms prior to the onset of motor findings (males, 16.5% vs. females 11.6%, p = 0.08). Other autonomic symptoms of this cohort have been described previously [10].
- More females endorsed incontinence (68.1%) than males (50.6%; p < 0.001), while males endorsed hesitancy (24.2% vs. 10.9%, p < 0.001) and incomplete emptying (31.2% vs. 18.4%, p < 0.001) more frequently than females. There was no sex difference in urgency (Figure 1B).
- Measurement of postvoid residual
- The proportion of males versus females who underwent PVR measurement was equal (27.0% vs. 27.7%, p = 0.839) (Figure 1C). The distribution of time to measurement of PVR from onset of urinary symptoms for both males and females was skewed to the right; over 40% of all evaluated patients underwent their evaluation within the first 18 months of symptoms (median time 1.5 years for males vs. 1.7 in females). Males and females who were already catheterized accounted for 14.6% and 12.1% of PVR measurements for their groups, respectively, and removal of their measurements from the analysis did not significantly change statistical findings. Thirty-eight patients had PVR measured by ultrasound, while 144 patients underwent catheterized PVR measurement. There was no sex difference in whether PVR was obtained with ultrasound or by catheterized samples (p = 0.311).
- Males were significantly more likely to have an elevated PVR (> 100 mL) than females (72.9% vs. 50.5%, p = 0.002) (Figure 1D). Males also had a larger average log-transformed PVR (males, 2.1 ± 0.1 vs. females, 1.9 ± 0.1; p = 0.0314) (Figure 1E). There was no difference in average log-transformed PVR among males without or with a comorbid diagnosis of BPH (2.1± 0.1 vs. 2.2 ± 0.1; p = 0.39; data not shown).
- Catheterization
- Catheterization rates were significantly lower in patients who were followed up for less than 90 days than in those who were followed up for 90 days or more (22.5% vs. 34.2, p < 0.001). However, there was no difference in the average log-transformed time to catheterization from the onset of urinary symptoms (< 90 days, 0.19 ± 0.05 vs. ≥ 90 days, 0.26 ± 0.06 years, p = 0.3204).
- While 16.0% of male patients were catheterized before evaluation at our institution, only 6.4% of females were already catheterized (p < 0.001). Overall, males were significantly more likely to be catheterized than females (35.1% vs. 17.3%, p < 0.001) (Figure 1F). When stratified by PVR, catheterization rates were similar between males and females when PVR was normal (15.4% vs. 8.9%, p = 0.4043) and when PVR was elevated (71.4% vs. 58.7%, p = 0.1556). When no PVR was measured (males, n = 260 vs. females, n = 238), males were more than twice as likely to be catheterized (27.3% vs. 10.9%, p < 0.001).
RESULTS
- Our findings confirm that urinary symptoms are highly prevalent among patients with MSA. We found differences in the type of urinary symptoms endorsed by male and female patients, likely a reflection of their underlying biological differences. We also found differences in PVR volumes between the sexes, likely suggesting biological differences. We found intriguing differences in referral and management patterns for urinary symptoms between sexes, which appeared to influence catheterization rates.
- Previous research from our group identified a higher catheterization rate in male patients with MSA [9]. We found that this difference is driven by patients who do not undergo measurement of PVR, a group in which males are twice as likely to be catheterized than females. Alternatively, when patients with MSA are referred for PVR measurement, there is no sex difference in catheterization rates: as would be expected, they are similarly low when PVR is not elevated and higher when it is. This is in line with recommendations for medical therapy in patients without elevated PVR [11] and clean intermittent catheterization for those with elevated PVR (> 100) [12]. Thus, as they do not influence catheterization rates in a sex-based manner, urodynamic studies could provide a standardized evaluation of lower urinary tract dysfunction.
- Our findings show that males are more likely to endorse hesitancy and incomplete emptying and have a higher PVR than females. Previous studies in MSA have suggested detrusor overactivity, acontractile detrusor, intrinsic sphincter deficiency, and detrusor-sphincter dyssynergia as causes of urinary dysfunction [13], and perhaps anatomical sex differences that impact pathophysiology.
- Incontinence is prevalent in elderly individuals, affecting an estimated 45%–78% of female versus 36%–75% of male nursing home residents with a mean age of 80–85 years. Unfortunately, systematic reviews have not been successful in identifying a sex difference in urinary incontinence in the general population due to broad definitions of the condition [14]. Although incontinence, a severe symptom on the spectrum of urinary dysfunction, was reported more frequently by the female patients in our cohort, there was no difference between males and females in referral rates for measurement of PVR. There are significant consequences for untreated urinary incontinence. Despite the degree to which it is underreported and undertreated, incontinence is associated with poor subjective quality of life [15]. Weekly episodes of urinary urge incontinence in the elderly general population significantly increase the risk of falls and nonspinal fractures, risks which are already elevated in people with prominent motor dysfunction such as MSA patients [16]. Despite this, it is estimated that just half of female patients seek care for their urinary incontinence, suggesting minimization of this symptom by patients and providers alike, and reinforcing the importance of inquiring about urinary symptoms in patients with MSA, regardless of sex [17-19].
- Our large, single-center cohort of MSA patients is a strength that permits evaluation of sex differences in urinary dysfunction and its management. One limitation is that most patients did not have long-term follow-up, yet analysis of both short- and long-term patients allows us to evaluate practice patterns between those seen on a consultative basis versus those followed through their disease process. Our study cohort includes a significantly higher proportion of catheterized patients who were followed for a longer period. As such, our study has revealed that as the disease progresses, urinary symptoms may increase, requiring changes in management [12]. There was no difference in time from urinary symptom onset to catheterization between groups, suggesting that our practice is similar to referring providers. Additionally, the difference in the percentage of males compared to females who are already catheterized at presentation to our center suggests that sex differences in treatment are also prominent at other centers. However, this should be evaluated further with a multicenter approach.
- Another limitation that must be considered is the absence of an age-matched healthy control cohort for comparison. Urinary symptoms are prevalent in the aging population, and the etiology may be multifactorial, including BPH in males and pelvic floor dysfunction in females. However, the significant failure rates of interventions directed at these suspected etiologies implicates alternative pathology. Furthermore, regardless of the role of sex in urinary symptoms in the normal aging population, the fact that females were referred less than males relative to the frequency of severe symptoms implies that we approach urinary symptoms differently depending on whether the patient presents as male or female and should prompt further consideration.
- The absence of self-identified gender in our cohort limits the application of these findings to the diversity of gender identities but does provide an opportunity to further characterize the effect of gender identity on urinary symptoms in neurodegenerative diseases in the future. However, the fundamental differential in allocation of care implicitly invokes societal understanding of sex differences, and thus, the concept of gender cannot be isolated from consideration of this topic.
- In summary, our findings detail differences that seem to be driven by biological sex (PVR volumes), societal influences of gender (referral for PVR measurement), and the relationship between the two (types of urinary symptoms that are reported), all of which ultimately influence diagnosis and management.
DISCUSSION
-
Data Sharing
The anonymized dataset will be shared with any qualified investigator upon request.
-
Conflicts of Interest
All authors have no financial disclosures or conflicts of interest for the preceding 12 months.
-
Funding Statement
This work was supported by CTSA Grant Number UL1 TR002377, Dominium Foundation Career Development Award in Neurodegenerative Disease Research in memory of Jack W. Safar from the National Center for Advancing Translational Science (NCATS), NIH (R01 NS092625, UL1 TR000135), Michael J. Fox Foundation, Bishop Dr. Karl Golser Foundation, Sturm Foundation, Mayo Center for Regenerative Medicine, and Mayo Funds.
-
Author Contributions
Conceptualization: Elizabeth A. Coon. Data curation: Elizabeth A. Coon. Formal analysis: Elke Schipani Bailey, Elizabeth A. Coon. Funding acquisition: Elizabeth A. Coon. Investigation: Elizabeth A. Coon. Methodology: Elke Schipani Bailey, Elizabeth A. Coon. Project administration: Elizabeth A. Coon. Supervision: Elizabeth A. Coon. Validation: Elke Schipani Bailey, Sara J. Hooshmand, Elizabeth A. Coon. Visualization: Elke Schipani Bailey, Elizabeth A. Coon. Writing—original draft: Elke Schipani Bailey. Writing—review & editing: all authors.
Notes
| Male (n = 356, 52.0%) | Female (n = 329, 48.0%) | p-value | ||
|---|---|---|---|---|
| Final diagnosis | 0.302 | |||
| MSA-P | 230 (64.6) | 200 (60.8) | ||
| MSA-C | 126 (35.4) | 129 (39.2) | ||
| Probable vs. Possible | 0.050 | |||
| Probable | 300 (84.3) | 294 (89.4) | ||
| Possible | 56 (15.7) | 35 (10.6) | ||
| Age at onset, avg (SEM) | 61.0 (0.5) | 61.9 (0.5) | 0.214 | |
| Time to diagnosis, yr | 4.2 (0.1) | 4.0 (0.1) | 0.350 | |
| Disease duration, yr | 7.7 (0.2) | 8.2 (0.2) | 0.084 | |
| Urinary symptoms | 327 (91.9) | 293 (89.1) | 0.212 | |
| Incontinence | 180 (55.0) | 224 (76.5) | < 0.001* | |
| Urgency | 150 (45.9) | 150 (51.2) | 0.185 | |
| Hesitancy | 79 (24.2) | 32 (10.9) | < 0.001* | |
| Incomplete emptying | 102 (31.2) | 54 (18.4) | < 0.001* | |
| Years from any MSA symptom onset to urinary symptom onset, avg (SEM) | 1.8 (0.2) | 2.2 (0.2) | 0.1674 | |
| Premotor onset | 54 (16.5) | 34 (11.6) | 0.08 | |
| Measurement of PVR | 96 (27.0) | 91 (27.7) | 0.839 | |
| Not previously catheterized | 82 (27.4) | 80 (26.0) | 0.686 | |
| PVR measurement type | 0.311 | |||
| PVR alone | 17 (17.7) | 21 (23.1) | ||
| Complete urodynamic study | 75 (78.1) | 69 (75.8) | ||
| Both | 4 (4.2) | 1 (1.1) | ||
| Follow up PVR measurement | 22 (22.9) | 14 (15.4) | 0.192 | |
| Postvoid residual > 100 | 70 (72.9) | 46 (50.5) | 0.002* | |
| Postvoid residual, median (IQR) | 204 (293) | 112 (206) | ||
| Postvoid residual, Log avg (SEM) | 2.1 (0.1) | 1.9 (0.1) | 0.0314* | |
| Not previously catheterized | 2.1 (0.1) | 1.9 (0.1) | 0.0244* | |
| Urinary catheterization | ||||
| All | 125 (35.1) | 57 (17.3) | < 0.001* | |
| No PVR performed | 71 (27.3) | 26 (10.9) | < 0.001* | |
| Prior to evaluation | 57 (16.0) | 21 (6.4) | < 0.001* | |
| PVR < 100 | 4 (15.4) | 4 (8.9) | 0.4043 | |
| PVR > 100 | 50 (71.4) | 27 (58.7) | 0.1556 | |
- 1. Gilman S, Wenning GK, Low PA, Brooks DJ, Mathias CJ, Trojanowski JQ, et al. Second consensus statement on the diagnosis of multiple system atrophy. Neurology 2008;71:670–676.ArticlePubMedPMC
- 2. Sakakibara R, Panicker J, Simeoni S, Uchiyama T, Yamamoto T, Tateno F, et al. Bladder dysfunction as the initial presentation of multiple system atrophy: a prospective cohort study. Clin Auton Res 2019;29:627–631.ArticlePubMedPDF
- 3. Institute of Medicine (US) Committee on Understanding the Biology of Sex and Gender Differences; Wizemann TM, Pardue ML. Exploring the biological contributions to human health: does sex matter? Chap. 6. The Future of Research on Biological Sex Differences: Challenges and Opportunities. [Internet] Washington (DC): National Academies Press (US); c2001, Jun [accessed on 2022 Apr 12]. Available at: https://www.ncbi.nlm.nih.gov/books/NBK222296/.
- 4. Bartz D, Chitnis T, Kaiser UB, Rich-Edwards JW, Rexrode KM, Pennell PB, et al. Clinical advances in sex-and gender-informed medicine to improve the health of all: a review. JAMA Intern Med 2020;180:574–583.ArticlePubMed
- 5. Jindal RM, Ryan JJ, Sajjad I, Murthy MH, Baines LS. Kidney transplantation and gender disparity. Am J Nephrol 2005;25:474–483.ArticlePubMedPDF
- 6. Mirin AA. Gender disparity in the funding of diseases by the US National Institutes of Health. J Womens Health (Larchmt) 2021;30:956–963.ArticlePubMedPMC
- 7. Pope JH, Aufderheide TP, Ruthazer R, Woolard RH, Feldman JA, Beshansky JR, et al. Missed diagnoses of acute cardiac ischemia in the emergency department. N Engl J Med 2000;342:1163–1170.ArticlePubMed
- 8. Zagni E, Simoni L, Colombo D. Sex and gender differences in central nervous system-related disorders. Neurosci J 2016;2016:2827090.ArticlePubMedPMCPDF
- 9. Coon EA, Nelson RM, Sletten DM, Suarez MD, Ahlskog JE, Benarroch EE, et al. Sex and gender influence symptom manifestation and survival in multiple system atrophy. Auton Neurosci 2019;219:49–52.ArticlePubMedPMC
- 10. Coon EA, Sletten DM, Suarez MD, Mandrekar JN, Ahlskog JE, Bower JH, et al. Clinical features and autonomic testing predict survival in multiple system atrophy. Brain 2015;138(Pt 12):3623–3631.ArticlePubMedPMC
- 11. Papatsoris AG, Papapetropoulos S, Singer C, Deliveliotis C. Urinary and erectile dysfunction in multiple system atrophy (MSA). Neurourol Urodyn 2008;27:22–27.ArticlePubMed
- 12. Ito T, Sakakibara R, Yasuda K, Yamamoto T, Uchiyama T, Liu Z, et al. Incomplete emptying and urinary retention in multiple-system atrophy: when does it occur and how do we manage it? Mov Disord 2006;21:816–823.ArticlePubMed
- 13. Bloch F, Pichon B, Bonnet AM, Pichon J, Vidailhet M, Roze E, et al. Urodynamic analysis in multiple system atrophy: characterisation of detrusor-sphincter dyssynergia. J Neurol 2010;257:1986–1991.ArticlePubMedPDF
- 14. Offermans MP, Du Moulin MF, Hamers JP, Dassen T, Halfens RJ. Prevalence of urinary incontinence and associated risk factors in nursing home residents: a systematic review. Neurourol Urodyn 2009;28:288–294.ArticlePubMed
- 15. Simeonova Z, Milsom I, Kullendorff AM, Molander U, Bengtsson C. The prevalence of urinary incontinence and its influence on the quality of life in women from an urban Swedish population. Acta Obstet Gynecol Scand 1999;78:546–551.ArticlePubMed
- 16. Gibson W, Hunter KF, Camicioli R, Booth J, Skelton DA, Dumoulin C, et al. The association between lower urinary tract symptoms and falls: forming a theoretical model for a research agenda. Neurourol Urodyn 2018;37:501–509.ArticlePubMedPDF
- 17. Minassian VA, Yan X, Lichtenfeld MJ, Sun H, Stewart WF. The iceberg of health care utilization in women with urinary incontinence. Int Urogynecol J 2012;23:1087–1093.ArticlePubMedPMCPDF
- 18. Kinchen KS, Burgio K, Diokno AC, Fultz NH, Bump R, Obenchain R et al. Factors associated with women’s decisions to seek treatment for urinary incontinence. J Womens Health (Larchmt) 2003;12:687–698.ArticlePubMed
- 19. Shaw C, Tansey R, Jackson C, Hyde C, Allan R. Barriers to help seeking in people with urinary symptoms. Fam Pract 2001;18:48–52.ArticlePubMed
REFERENCES
Figure & Data
References
Citations
- In vivo cerebral metabolic and dopaminergic characteristics in multiple system atrophy with orthostatic hypotension
Chenxi Xue, Xiaofeng Dou, Congcong Yu, Yan Zhong, Jing Wang, Xiang Zhang, Le Xue, Daoyan Hu, Shuang Wu, Hong Zhang, Mei Tian
European Journal of Nuclear Medicine and Molecular Imaging.2024; 51(2): 468. CrossRef
Comments on this article
 PubReader
PubReader ePub Link
ePub Link Cite
Cite
