1Department of Neurology, National Institute of Mental Health and Neurosciences (NIMHANS), Bengaluru, India
2Department of Neuroimaging and Intervention Radiology, National Institute of Mental Health and Neurosciences (NIMHANS), Bengaluru, India
Corresponding author: Vikram V. Holla, MD, DM Department of Neurology, National Institute of Mental Health and Neurosciences (NIMHANS), Hosur Rd, Lakkasandra, Bengaluru 560029, India / Tel: +91-80-26995488 / E-mail: vikramvholla@gmail.com
• Received: June 4, 2023 • Revised: July 18, 2023 • Accepted: August 2, 2023
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Isoniazid is an antitubercular drug that is an important part of the first-line treatment regimen for tuberculosis treatment and prophylaxis. Although hepatotoxicity is one of the common side effects of isoniazid, neurological complications such as encephalopathy, seizure, peripheral neuropathy, and occasional ataxia are not uncommon. Isoniazid-induced ataxia is often associated with bilateral dentate nucleus hyperintensity, with only a few reports of additional thalamic hyperintensity. We report a case of possible isoniazid toxicity-induced ataxia in a 23-year-old man in whom magnetic resonance imaging (MRI) of the brain showed bilateral thalamic hyperintensity along with the “face of the giant panda” sign.
A 23-year-old man presented with a two-week history of fever, headache, and vomiting. The examination was normal except for meningeal signs. MRI of the brain showed basal-predominant diffuse pachymeningeal enhancement and cerebrospinal fluid analysis revealed lymphocytic pleocytosis, elevated protein, and a positive test for rifampicin-sensitive mycobacterial tuberculosis detected on a cartridge-based nucleic acid amplification test (CBNAAT), confirming the diagnosis of tuberculous meningitis. The patient was initiated on four first-line drugs for the intensive phase of antitubercular treatment (ATT), consisting of a weight-appropriate dose of isoniazid (300 mg), rifampicin (600 mg), pyrazinamide (1,500 mg), and ethambutol (900 mg), along with 40 mg of pyridoxine. Complete recovery was noted over the next few weeks, and at the three-month follow-up, isoniazid, rifampicin, and ethambutol were continued. In the fourth month, the patient presented with subacute-onset walking difficulty and incoordination with a duration of 2 weeks. There were no other relevant symptoms, and the patient was not taking any medications apart from the continuation phase of ATT.
On examination, the patient was conscious, alert, and oriented and had horizontal gaze-evoked nystagmus, cerebellar dysarthria, impaired performance on the finger-nose and knee-heel-shin tests, ataxic gait, and impaired tandem walking (Figure 1, Segment 1 of Supplementary Video 1 in the online-only Data Supplement). The rest of the systemic and neurological examinations were normal. MRI of the brain revealed bilateral hyperintensity of the thalamus and the posterior limb of the internal capsule (PLIC) along with midbrain hyperintensity in the form of “face of the giant panda sign” (Figure 1A-E). Routine blood tests, including liver and renal function tests, were normal. Isoniazid toxicity was considered, and this drug was discontinued. There was no evidence of other features of isoniazid toxicity, such as hepatotoxicity, peripheral neurotoxicity, or skin hyperintensity. The patient was shifted over to the ATT regimen given for isoniazid-resistant tuberculosis, composed of rifampicin (600 mg), ethambutol (900 mg), pyrazinamide (1,500 mg) and moxifloxacin (400 mg), and pyridoxine was continued. Three months after discontinuation of isoniazid, both clinical and radiological resolution were noted, thereby substantiating the possibility that the observed ataxia and MRI brain changes had been related to isoniazid toxicity (Figure 1F-J, Segment 2 of Supplementary Video 1 in the online-only Data Supplement). However, we could not assess isoniazid blood levels due to the nonavailability of the test.
Isoniazid toxicity is classically associated with dentate nucleus hyperintensity, with rare reports of thalamic hyperintensity [1,2] and no reports of either hyperintensity of the PLIC or giant panda sign. The toxic effect of isoniazid on myelin has been demonstrated in laboratory animals in the form of rapidly reversible vacuolation, possibly due to oxidative stress and lipid peroxidation [3]. The prompt resolution after cessation of isoniazid substantiates the reversible nature of this vacuolation [1]. The high myelin content of the thalamus, PLIC, and midbrain may explain their involvement in this case.
Bilateral thalamic involvement can be seen due to a wide range of causes, such as artery of Percheron infarction, deep venous sinus thrombosis, flavivirus encephalitis, Creutzfeldt‒Jakob disease, various inborn errors of metabolism, Wilson disease, Wernicke encephalopathy and hypoxic ischemic encephalopathy. The face of the giant panda sign, initially identified in neurological Wilson’s disease [4] and considered to be a specific finding in Wilson’s disease, has also been reported in Japanese encephalitis, hypoxic ischemic encephalopathy, Leigh’s disease, maple syrup urine disease, non-Wilsonian hepatolenticular degeneration, and, recently, central nervous system lymphoma [5-7]. The hyperintensity of the midbrain tegmentum with preserved hypointensity of the red nucleus (eyes), lateral part of the substantia nigra pars reticulata (ears) and superior colliculus (chin) comprises the face of the giant panda sign.
In conclusion, isoniazid toxicity should be considered as one of the differential diagnoses for MRI findings of bilateral thalamic hyperintensity and face of the giant panda sign. Discontinuation of isoniazid in such cases results in prompt reversal of clinical and radiological abnormalities.
Baseline and the follow-up video of the patient. Segment 1: Video of the patient at baseline showing dysarthria, impaired finger-nose and knee-heel-shin test, ataxic gait and impaired tandem walking. Segment 2: These signs were resolved as of the 3-month follow-up
Notes
Ethics Statement
The authors confirm that the an Institution Ethics Committee review waiver was obtained from the institutional review board of National Institute of Mental Health and Neurosciences for the work (NIMHANS/IEC/2023). We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this work is consistent with those guidelines. The video of the patient was taken after written informed consent was obtained for publication and dissemination.
Conflicts of Interest
The authors have no financial conflicts of interest.
Funding Statement
None
Author contributions
Conceptualization: Vikram V. Holla, Pramod Kumar Pal. Data curation: Vikram V. Holla, Manjunath Netravathi, Jitender Saini. Formal analysis: Vikram V. Holla. Investigation: all authors. Visualization: Vikram V. Holla, Manjunath Netravathi, Pramod Kumar Pal. Writing—original draft: Vikram V. Holla. Writing—review & editing: Manjunath Netravathi, Nitish Kamble, Jitender Saini, Pramod Kumar Pal.
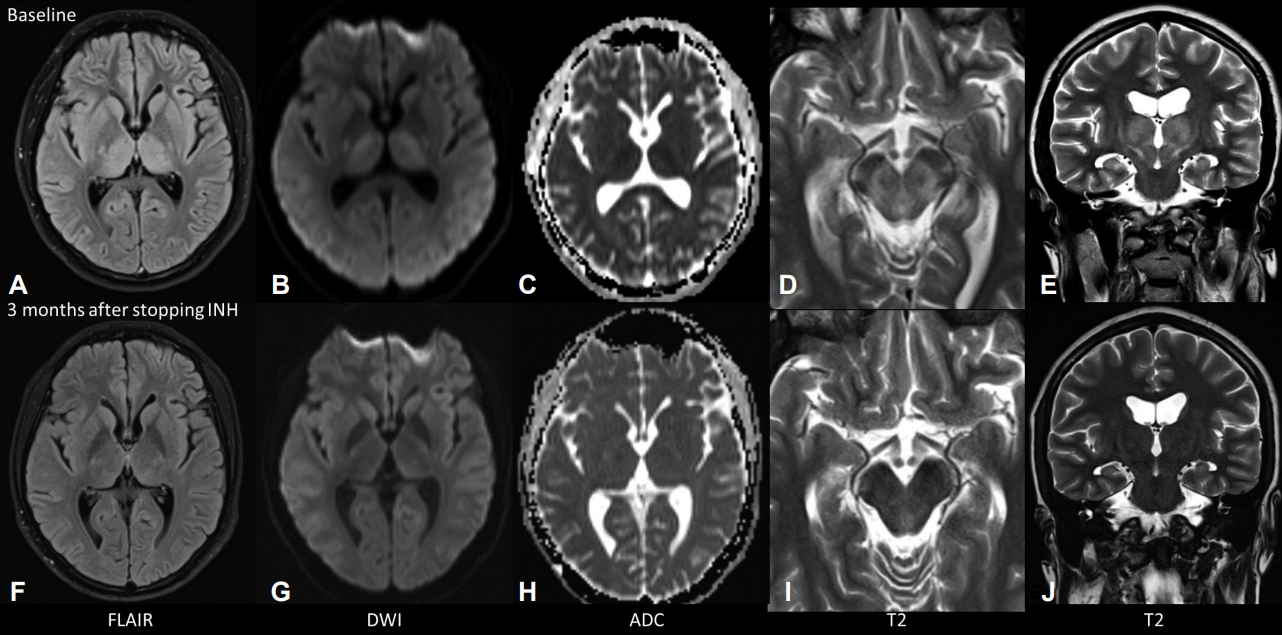
Figure 1.
MRI of the brain at baseline showing bilateral hyperintensity of the thalamus and the posterior limb of the internal capsule (A, E) with diffuse restriction (B, C) and “face of the giant panda sign” (D). At the 3-month follow-up after cessation of isoniazid, these findings were found to be completely resolved (F-J). MRI, magnetic resonance imaging; INH, isoniazid; ADC, apparent diffusion coefficient; DWI, diffusion weighted imaging; FLAIR, fluid attenuated inversion recovery.
REFERENCES
1. Hawkes M, Kitai I, Blaser S, Cohen E, Bitnun A, Fluss J, et al. Neuroimaging findings in isoniazid central nervous system toxicity, presumed intramyelinic edema. Eur J Paediatr Neurol 2008;12:512–515.ArticlePubMed
2. Hasiloglu ZI, Albayram S, Asik M, Kilic O, Unver O, Erdemli HE, et al. MRI findings of isoniazid-induced central nervous system toxicity in a child. Clin Radiol 2012;67:932–935.ArticlePubMed
3. Schmued LC, Albertson CM, Andrews A, Sandberg JA, Nickols J, Slikker W Jr. Evaluation of brain and nerve pathology in rats chronically dosed with ddI or isoniazid. Neurotoxicol Teratol 1996;18:555–563.ArticlePubMed
4. Hitoshi S, Iwata M, Yoshikawa K. Mid-brain pathology of Wilson’s disease: MRI analysis of three cases. J Neurol Neurosurg Psychiatry 1991;54:624–626.ArticlePubMedPMC
5. Sharawat IK, Kochar GS, Saini AG, Sankhyan N. “Face of the giant panda” sign and temporal cystic changes in maple syrup urine disease. Indian J Pediatr 2019;86:755–756.ArticlePubMedPDF
6. Vella S, Grech R. Highlighting an atypical cause of the face of the giant panda sign. BJR Case Rep 2017;4:20170046.ArticlePubMedPMC
7. Kim JY, Choi JH, Oh EH, Choi SY, Kim HJ, Choi KD. Isolated vestibular syndrome with “double-panda” sign in CNS lymphoma. J Clin Neurol 2022;18:111–113.ArticlePubMedPMCPDF
 E-submission
E-submission

 , Manjunath Netravathi1
, Manjunath Netravathi1
 PubReader
PubReader ePub Link
ePub Link Cite
Cite
