 E-submission
E-submission
Articles
- Page Path
- HOME > J Mov Disord > Volume 13(2); 2020 > Article
-
Review Article
Nutrition and Lifestyle Interventions for Managing Parkinson’s Disease: A Narrative Review -
Tracy Lister

-
Journal of Movement Disorders 2020;13(2):97-104.
DOI: https://doi.org/10.14802/jmd.20006
Published online: May 29, 2020
Maryland University of Integrative Health, Laurel, MD, USA
- Corresponding author: Tracy Lister, DCN Maryland University of Integrative Health, 7750 Montpelier Road, Laurel 20723, MD, USA / Tel: +1-250-954-7908 / E-mail: nutrition.endeavors@gmail.com
• Received: January 24, 2020 • Revised: March 3, 2020 • Accepted: March 17, 2020
Copyright © 2020 The Korean Movement Disorder Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
- The etiology of Parkinson’s disease (PD) is not fully understood, but environmental toxin overexposure, increased intestinal permeability, and dysbiosis related to nutrition and lifestyle habits are thought to be contributors. Considering these nutrition and lifestyle implications, there is a lack of practice-based programs utilizing interventions for managing symptoms or slowing the progression of the disease. The purpose of this narrative review was to identify relevant research related to nutrition and lifestyle interventions for PD, evaluate the research utilizing the evidence analysis process of the Academy of Nutrition and Dietetics to assess the quality of each research article, and group the research into categories. A grading of recommendations assessment, development and evaluation (GRADE) of either good, fair, limited, or not assignable was allocated to each category of research, including diet patterns, vitamin D, B-complex, omega-3 fatty acids, coenzyme Q10, probiotics, physical activity, stress, and sleep. An intervention based on the research presented in the review may be utilized for coaching people with PD on symptom management.
- The analysis process utilized to write the review is described in the Academy of Nutrition and Dietetics (AND) 2012 Evidence Analysis Manual [28]. During September 2019, PubMed and EbscoHost were searched for literature utilizing 42 search words related to nutrition and lifestyle AND/OR Parkinson resulting in 42 individual searches (Table 1). Database filters consisted of human studies, English language, and primary research/peer publications. The exclusion criteria included animal or in vitro studies, case studies, narrative reviews, gene therapy, risk of developing PD, and pharmaceutical research. Each article meeting the inclusion criteria was assessed for quality utilizing the AND checklists; those graded as negative quality were also excluded. The research articles were then grouped into categories, and each category was assigned a grading of recommendations assessment, development and evaluation (GRADE) with a definition and conclusion statement (Figure 1). There was only one reviewer evaluating the quality of each individual research article, grouping the positive and neutral quality articles into categories and arbitrarily assigning a GRADE to each category based on the quantity and quality of the research.
MATERIALS & METHODS
- Utilizing key words AND Parkinson produced 6,045 publications, of which 56 were considered relevant, with 41 assigned a neutral or positive quality rating; these were then grouped into the categories of diet patterns, vitamin D, omega-three fatty acids (n-3), B vitamins, coenzyme Q10 (CoQ10), probiotics, physical activity (PA), sleep, and stress. Research on stress management with regard to PD was lacking, with only one study utilizing yoga as the intervention.
- The collection of research related to diet patterns was assigned a GRADE of fair (II) due to utilizing study designs that are less appropriate for interventions (cohort, crossover) and small sample sizes. However, designing ethical nutrition and health research is difficult, and studies regarding diet patterns and organic plant-based food items are compelling [29-31]. The Mediterranean-DASH Diet Intervention for Neurodegenerative Delay (MIND) diet, studied to reduce neurodegenerative changes, was associated with a 13% reduction in the risk of developing PD or the progression of symptoms. It is a Mediterranean-type plant-based anti-inflammatory diet consisting of vegetables, fruits, legumes, whole grains, nuts, small wild fish, and small amounts of farm raised poultry and red meats low in saturated fats [31]. Considering that PD is related to toxic burden, a plant-based diet, which is high in vegetables and some fruits, should consist mostly of organic foods. Lu et al. [30] conducted a study to determine the contribution of pesticide intake from vegetables and fruits in American children at a private school. The pesticides malathion dicarboxylic acid and malathion tricholoro-2 pyridinol were detected in the children’s urine on days they were fed their usual diet but not the days they were fed an organic diet.
- Organic plant-based diets tend to be lower in protein due to limiting or excluding animal foods; therefore, supplementing with a protein powder may be necessary to meet protein requirements. Supplementing with 20 g of organic whey protein powder daily has been shown to improve motor function, reduce homocysteine related to inflammation, and increase glutathione synthesis necessary for detoxification in those with PD [32]. Higher protein diets such as a ketogenic or gluten-free diet have been proposed as interventions for PD, as studies show improvements in motor function due to better glycemic control and reduced toxicity associated with food intolerances [33,34].
- Several nutrition supplements related to PD have been investigated, but there was a lack of high-quality studies utilizing vitamin D. Vitamin D supplementation research provides conflicting results regarding PD, which may be related to the dose provided and the length of the studies. A prospective cohort in China found that 43% of participants with PD had lower serum levels than controls, which trended towards a positive correlation with disease duration [35]. Hiller et al. [36] reported significant improvements in balance when participants with PD were supplemented with 10,000 IU vitamin D daily. Another trial supplementing 1,200 IU daily for 12 months in those with serum levels of 22.5 ± 9.7 ng/mL reported improved PD symptoms when serum levels reached 41.7 ± 12.6 ng/mL [37].
- There are only two trials with the same small sample utilizing 1,000 mg of n-3s from flaxseed oil for 12 weeks. These studies reported a reduction in inflammatory markers and increased antioxidative capacity and glutathione production, reducing PD symptoms [38,39].
- There are a limited number of studies utilizing individual B vitamins and deficiency states in PD. Thiamine (B1) deficiency has been linked with neuroinflammation and neurodegeneration, suggesting a role in the progression of PD [40]. An observational study found that 100 mg of B1 administered intramuscularly twice weekly improved PD symptoms within 3 months [40]. Coimbra et al. [41] conducted a study to determine the riboflavin (B2) status among participants with PD and found that people with PD had lower serum B2 levels compared to controls. After supplementation with 30 mg of B2 every eight hours, participants reported improved sleep, reasoning, and motivation and reduced depression within two weeks and improved motor function by 44–71% in three months. A deficiency in B vitamins is associated with neuroinflammation and oxidative stress, for which homocysteine is a biomarker [42]. Ozer et al. [43] found a negative correlation between homocysteine and visual-spatial tasks, learning, serum vitamin B12, and serum folate.
- People with PD tend to be at greater odds of a CoQ10 deficiency, an antioxidant that is important for the detoxification system, which may be partially responsible for their toxic burden [44]. Several high-quality studies have shown that supplementation with 100–1,200 mg of CoQ10 daily, particularly larger dosages, reduces inflammatory markers and improves motor symptoms [45-49].
- There is very little research regarding interventions to support a healthy microbiome in PD. A study with participants with PD utilizing fermented milk rich in probiotics combined with a prebiotic fiber reduced incomplete evacuation of stool and increased the frequency from 3 to 4.5 bowel movements weekly [50]. A trial conducted with probiotic supplements containing 8 × 109 CFU reduced inflammatory markers, but changes in PD symptoms were not tracked [51]. Abnormalities in the microbiota may extend to the esophagus and oropharyngeal cavity, which may be related to a higher number of alpha-synuclein mutations found in the oral cavity of subjects with PD [14]. It has been speculated that these abnormalities may be responsible for PD nonmotor symptoms, including changes in swallowing, taste, smell, salivation, and speech.
- There was a wealth of publications related to PA. Many studies utilized the American College of Sports Medicine (ACSM) guidelines, suggesting that people engage in 150 minutes of moderate-intensity PA weekly or 75 minutes of high-intensity training or a combination of both [52]. Several studies with PA utilizing the ACSM guidelines found that higher intensity exercise improves motor function, balance, cognition, depression, sleep, and quality of life [53-58]. Two studies showed an improvement in inflammatory markers, and Landers et al. [59] reported improved motor and nonmotor skills and neuroplasticity [60]. Corcos et al. [61] reported that progressive weightlifting improved motor skills more than a nonprogressive program.
- Other forms of exercise, such as yoga, tai chi (TC), and dance, have led to improvements in motor and nonmotor function. Yoga has been shown to improve sleep, depression, cognition, balance, motor skills, and quality of life [62-64]. TC improves not only motor skills but also flexibility, internal awareness, orientation, and proprioception [65-67]. Hackney and Earhart [68] reported that tango had a larger impact on motor skills than TC, which may be related to the impact of music and rhythm and the increased cognitive demands of memorizing steps and motor planning.
- There was a lack of published research related directly to PD and sleep and stress. Inadequate or ineffective sleep impacts the brain and motor skills, which may be related to replenishing dopamine levels [69,70]. Research specifically related to PD and stress was limited to one small study with 10 participants with PD reporting a reduction in psychological stress and increased wellbeing [71].
RESULTS
- The evidence suggests that nutrition and lifestyle interventions may reduce PD symptoms and possibly delay disease progression. Prescribing specific diet patterns and nutritional supplements has the potential to reduce inflammation and toxin exposure, support detoxification, heal the gut, and calm the immune system to reduce PD symptoms and promote health and wellbeing.
- The research supports prescribing a Mediterranean-type diet pattern to reduce inflammation by focusing on whole foods that are low in toxins [31]. The diet pattern is high in vitamins, minerals, fiber, and antioxidants, including flavonoids, which are found in plant-based foods, particularly berries. Gao et al. [72] in their cohort study reported reduced risk and progression of PD with the consumption of flavonoids as these antioxidants cross the blood brain barrier, reduce inflammation, influence neural signaling, and improve the survival of dopamine neurons. Curcumin/turmeric should be included as a spice in cooking due to its antioxidant abilities that protect cells, restore cell morphological changes, increase cell survival, and reduce cell death by influencing gene expression [73,74].
- Food sensitivities and intolerances often go undetected, which may contribute to toxic burden, inflammation, and gut damage leading to excessive immune responses. There appears to be a connection between PD and celiac disease, suggesting the possibility of nonceliac gluten intolerance, which may cause cerebellar ataxia and neuropathy [34,75]. A systematic review conducted in 2018 suggested that gluten sensitivity should be considered for movement disorders owing to the connection with neurological dysfunction [76]. Therefore, an elimination diet should be tried for people with PD to identify any possible food sensitivities or intolerances that are contributing to symptoms. Once food sensitivities have been identified, a modified Mediterranean-type diet should be prescribed for long-term usage.
- Avoiding processed foods, sugar and sugar substitutes will reduce inflammation and toxic burden and improve blood glucose in most individuals, which is essential for supporting neurological health [33]. Excess carbohydrate intake may also interfere with muscle protein synthesis, reducing muscle strength and function [77].
- Obtaining adequate protein sources may be challenging due to locating organic meats and poultry and wild fish. Supplementing with 20 g of whey protein spread throughout the day preserves muscle mass and reduces oxidative stress and inflammation [32]. Whey protein is a good source of cysteine that is needed for glutathione production to support detoxification and reduce homocysteine. As glutathione appears to be ineffective as a supplement, food sources are required to increase its biosynthesis to reduce inflammation and oxidative damage to neurons [32].
- Diet and gut health also play an important role in supporting detoxification and managing constipation [78]. Regular bowel movements prevent toxins from deconjugating and being freed within the lumen and reabsorbed in the presence of increased intestinal permeability [78,79]. Fiber binds toxins and influences tight junction proteins that support gut wall integrity to prevent increased intestinal permeability and toxin reabsorption [78-80]. Substances that alter the microbiome and damage the gut include medications, a low-fiber diet high in processed foods, infectious agents and food intolerances [81,82]. Gut dysbiosis is a result of consuming foods that are poorly tolerated or highly processed, leading to an overgrowth of gram-negative bacteria and their inflammatory byproducts. It has been well established that an altered microbiota is prevalent in PD [2,13,81].
- PA is an important aspect of managing PD and should include a variety of activities. Most types of PA are beneficial, but the key is motivation; therefore, the activity chosen should be enjoyed [58]. Even though all forms of PA appear to improve PD, each type of activity has its own unique benefits. An exercise program that is guided by a professional to increase exertion over time is more effective at improving motor skills and balance compared to nonprogressive programs [53-61]. Interval training with high spurts of activity followed by lower exertion activities has the best outcomes, including neuroplasticity, which includes improving cognition and mental health [53,54]. An exercise routine of stretching, strength training and aerobic activity improves depression and quality of life, which might be related to increasing brain-derived neurotrophic factor and decreasing inflammation [57,59,60]. Strength training combined with an adequate intake of dietary protein is important not only for managing PD symptoms but also for reducing age-related sarcopenia associated with frailty [32,83].
- Yoga, dance, and TC may be more enjoyable than regimented PA programs for some individuals and more appropriate for the elderly or those with limited motor function [62,64-67,84,85]. Yoga is beneficial for improving motor function, overall physical fitness, flexibility, strength, sleep, and stress [62,64,71]. Dancing provides not only a social experience but also improves intellectual function, flexibility, balance, strength, functional movements (including finger and hand dexterity), motor planning and memory in people with PD [84]. TC improves quality of life and depression [67].
- Sleep is important for PD management as it improves motor function possibly by restoring dopamine levels [70,86]. Ineffective sleep also has a negative impact on brain and motor skills, worsening symptoms and quality of life. Although the effects of sleep on PD are not well studied, the research does support a positive effect of sleep on other neurological diseases and motor skill improvements even in healthy individuals [69,87].
- There are no high-quality studies linking stress and PD, but it is well known that stress has a direct connection to developing chronic diseases, particularly those of the brain [88]. Chronic stress affects neuropeptide signaling, causing anxiety, depression, and inflammation related to disease. The dopaminergic nuclei are also inhibited by chronic stress, which may be related to the depressive symptoms common in PD. Depression may affect glutamate, which activates receptors and alters the hippocampal excitatory synapse, which affects cognition, another common feature of PD. Stress reduction should be addressed in the management of PD, as it has the potential to reduce symptoms and improve overall health and quality of life.
- Research suggests that people with PD are deficient in CoQ10, glutathione and vitamins C and D [35,44,88,90]. Coenzyme Q10 at dosages of 300–1,200 mg daily may have a positive impact on motor neuron symptoms, finger dexterity, visual color acuity, and inflammation. Glutathione is not beneficial as a supplement, but its endogenous production relies on nutrients provided by a Mediterranean-type diet high in cruciferous and allium vegetables, citrus, and berries and possibly supplemental n-acetyl cysteine [91]. A small study administering large dosages of oral nacetyl cysteine (1,200 to 8,000 mg/day) to five participants with PD reported an increase in serum glutathione without adverse effects at a dose of 1,200 mg daily [92].
- People with PD are at risk of vitamin D deficiency, but there is conflict in the research regarding the daily dose [35,36,93]. The impact of adequate vitamin D for good health is well established; therefore, serum levels should be tested and treated as needed [94]. To treat deficiencies, calculating a dose based on 40 IU for every 12 ng/mL for serum levels below 50 ng/mL may be the best approach [95].
- Although there is no research related to PD and vitamin C supplementation, vitamin C is a powerful antioxidant that quenches reactive oxygen species developed during detoxification. Ide et al. [89] found an inverse relationship between serum vitamin C and the most severe stages of PD. As vitamin C supports detoxification, food sources would be included in the daily diet pattern.
- Deficiencies in B vitamins are more prevalent with PD than in the healthy population [40,96]. Deficiencies in B1 are linked with neuroinflammation and neurodegeneration and B12, B6, and folate to elevated homocysteine. Correcting B1 deficiency may improve motor function, fatigue and cognition [96]. Motor symptoms, sleep, motivation, and depression improve with the correction of B2 deficiency [41]. Correcting B6, B12 and folate deficiencies has a positive effect on homocysteine, which tends to be high in those taking levodopa [97]. In clinical practice, biomarkers of B vitamins have several limitations for assessing nutrition status; therefore, a thorough nutrition-focused physical examination should be conducted to identify micronutrient deficiencies that should then be treated as needed [98,99].
- Omega-three fatty acids reduce inflammation and may improve PD motor skills. Flaxseed is a source of n-3s, but the conversion of alpha-linolenic acid to eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) is very small; therefore, fish sources that are rich in EPA and DHA are recommended [100]. As fish are contaminated with methylmercury and polychlorinated biphenyl, prescribed n-3 supplements should be purified. The suggested dose is 1 g increasing to 4 g daily as tolerated [38,39].
- Consuming probiotic supplements and prebiotics as food sources reduces inflammation and oxidative stress to heal the gut and correct the balance of microbes. As there is limited information regarding specific strains for PD, supplementation with 8 × 109 CFU live bacteria with a variety of species is a general recommendation based on the available research.
- A systematic search of the literature has provided research regarding diet patterns, supplements, and PA, with limited research on probiotics, vitamin C, individual B vitamins and the impact of sleep and stress on PD. Another limitation of the literature review is that a single author evaluated the literature and assigned a GRADE to categories of research. Regardless of the limitations, the research suggests that providing nutrition and lifestyle interventions for people with PD or parkinsonism symptoms may be beneficial. Future research is needed to identify the potential benefits of nutrients with limited research identified in this review. A program including a Mediterranean-type diet, supplements, stress management and sleep hygiene needs to be developed and tested as a pilot program to determine the impact on quality of life and disease progression.
DISCUSSION
- None.
Acknowledgments
Figure 1.Grade definitions: strength of evidence for a conclusion statement. Adapted from Academy of Nutrition and Dietetics.[28]
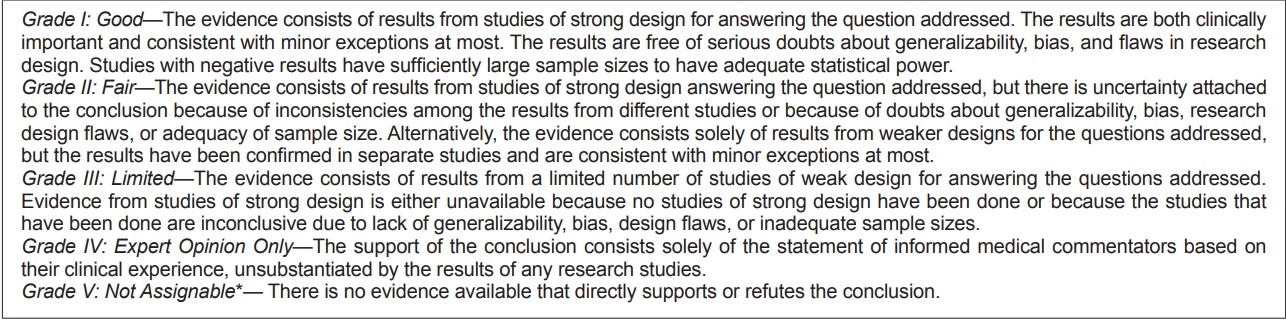
Table 1.Literature search terms, categories of topics and GRADEs
- 1. Tysnes OB, Storstein A. Epidemiology of Parkinson’s disease. J Neural Transm (Vienna) 2017;124:901–905.ArticlePubMedPDF
- 2. Lin CH, Chen CC, Chiang HL, Liou JM, Chang CM, Lu TP, et al. Altered gut microbiota and inflammatory cytokine responses in patients with Parkinson’s disease. J Neuroinflammation 2019;16:129.ArticlePubMedPMCPDF
- 3. Postuma RB, Gagnon JF, Pelletier A, Montplaisir J. Prodromal autonomic symptoms and signs in Parkinson’s disease and dementia with Lewy bodies. Mov Disord 2013;28:597–604.ArticlePubMed
- 4. Eisenhofer G, Aneman A, Friberg P, Hooper D, Fåndriks L, Lonroth H, et al. Substantial production of dopamine in the human gastrointestinal tract. J Clin Endocrinol Metab 1997;82:3864–3871.ArticlePubMed
- 5. Houser MC, Tansey MG. The gut-brain axis: is intestinal inflammation a silent driver of Parkinson’s disease pathogenesis? NPJ Parkinsons Dis 2017;3:3.ArticlePubMedPMCPDF
- 6. Hilton D, Stephens M, Kirk L, Edwards P, Potter R, Zajicek J, et al. Accumulation of α-synuclein in the bowel of patients in the pre-clinical phase of Parkinson’s disease. Acta Neuropathol 2014;127:235–241.ArticlePubMedPDF
- 7. Caputi V, Giron MC. Microbiome-gut-brain axis and Toll-like receptors in Parkinson’s disease. Int J Mol Sci 2018;19:1689.ArticlePubMedPMC
- 8. Mittal R, Debs LH, Patel AP, Nguyen D, Patel K, O’Connor G, et al. Neurotransmitters: the critical modulators regulating gut-brain axis. J Cell Physiol 2017;232:2359–2372.ArticlePubMedPMC
- 9. Houser MC, Chang J, Factor SA, Molho ES, Zabetian CP, Hill-Burns EM, et al. Stool immune profiles evince gastrointestinal inflammation in Parkinson’s disease. Mov Disord 2018;33:793–804.ArticlePubMedPMC
- 10. Knudsen K, Fedorova TD, Bekker AC, Iversen P, Østergaard K, Krogh K, et al. Objective colonic dysfunction is far more prevalent than subjective constipation in Parkinson’s disease: a colon transit and volume study. J Parkinsons Dis 2017;7:359–367.ArticlePubMed
- 11. Salat-Foix D, Tran K, Ranawaya R, Meddings J, Suchowersky O. Increased intestinal permeability and Parkinson disease patients: chicken or egg? Can J Neurol Sci 2012;39:185–188.ArticlePubMed
- 12. Umemura A, Oeda T, Yamamoto K, Tomita S, Kohsaka M, Park K, et al. Baseline plasma C-reactive protein concentrations and motor prognosis in Parkinson disease. PLoS One 2015;10:e0136722.ArticlePubMedPMC
- 13. De Filippis F, Pellegrini N, Laghi L, Gobbetti M, Ercolini D. Unusual subgenus associations of faecal Prevotella and Bacteroides with specific dietary patterns. Microbiome 2016;4:57.ArticlePubMedPMCPDF
- 14. Mihaila D, Donegan J, Barns S, LaRocca D, Du Q, Zheng D, et al. The oral microbiome of early stage Parkinson’s disease and its relationship with functional measures of motor and non-motor function. PLoS One 2019;14:e0218252.ArticlePubMedPMC
- 15. Steenland K, Wesseling C, Román N, Quirós I, Juncos JL. Occupational pesticide exposure and screening tests for neurodegenerative disease among an elderly population in Costa Rica. Environ Res 2013;120:96–101.ArticlePubMed
- 16. Narayan S, Liew Z, Paul K, Lee PC, Sinsheimer JS, Bronstein JM, et al. Household organophosphorus pesticide use and Parkinson’s disease. Int J Epidemiol 2013;42:1476–1485.ArticlePubMedPMCPDF
- 17. Caballero M, Amiri S, Denney JT, Monsivais P, Hystad P, Amram O. Estimated residential exposure to agricultural chemicals and premature mortality by Parkinson’s disease in Washington State. Int J Environ Res Public Health 2018;15:2885.ArticlePubMedPMC
- 18. Gorell JM, Johnson CC, Rybicki BA, Peterson EL, Kortsha GX, Brown GG, et al. Occupational exposure to manganese, copper, lead, iron, mercury and zinc and the risk of Parkinson’s disease. Neurotoxicology 1999;20:239–247.PubMed
- 19. Coon S, Stark A, Peterson E, Gloi A, Kortsha G, Pounds J, et al. Wholebody lifetime occupational lead exposure and risk of Parkinson’s disease. Environ Health Perspect 2006;114:1872–1876.ArticlePubMedPMC
- 20. Jiang W, Ju C, Jiang H, Zhang D. Dairy foods intake and risk of Parkinson’s disease: a dose-response meta-analysis of prospective cohort studies. Eur J Epidemiol 2014;29:613–619.ArticlePubMedPDF
- 21. Kamel F, Goldman SM, Umbach DM, Chen H, Richardson G, Barber MR, et al. Dietary fat intake, pesticide use, and Parkinson’s disease. Parkinsonism Relat Disord 2014;20:82–87.ArticlePubMed
- 22. Helley MP, Pinnell J, Sportelli C, Tieu K. Mitochondria: a common target for genetic mutations and environmental toxicants in Parkinson’s disease. Front Genet 2017;8:177.ArticlePubMedPMC
- 23. Müller T. Detoxification and antioxidative therapy for levodopa-induced neurodegeneration in Parkinson’s disease. Expert Rev Neurother 2013;13:707–718.ArticlePubMed
- 24. Inamdar AA, Hossain MM, Bernstein AI, Miller GW, Richardson JR, Bennett JW. Fungal-derived semiochemical 1-octen-3-ol disrupts dopamine packaging and causes neurodegeneration. Proc Natl Acad Sci U S A 2013;110:19561–19566.ArticlePubMedPMC
- 25. Schirinzi T, Martella G, D’Elia A, Di Lazzaro G, Imbriani P, Madeo G, et al. Outlining a population “at risk” of Parkinson’s disease: evidence from a case-control study. Parkinsons Dis 2016;2016:9646057.ArticlePubMedPMCPDF
- 26. Caudle WM, Guillot TS, Lazo CR, Miller GW. Industrial toxicants and Parkinson’s disease. Neurotoxicology 2012;33:178–188.ArticlePubMedPMC
- 27. Sheard J, Ash S. Current practice in nutrition diagnosis and intervention for the management of Parkinson’s disease in Australia and Canada. Nutrition & Dietetics 2015;72:30–35.Article
- 28. Academy of Nutrition and Dietetics. Evidence analysis manual: steps in the academy evidence process. Chicago, IL: Academy of Nutrition and Dietetics; 2016.
- 29. Heaney RP. Nutrients, endpoints, and the problem of proof. J Nutr 2008;138:1591–1595.ArticlePubMedPDF
- 30. Lu C, Toepel K, Irish R, Fenske RA, Barr DB, Bravo R. Organic diets significantly lower children’s dietary exposure to organophosphorus pesticides. Environ Health Perspect 2006;114:260–263.ArticlePubMed
- 31. Agarwal P, Wang Y, Buchman AS, Holland TM, Bennett DA, Morris MC. MIND diet associated with reduced incidence and delayed progression of parkinsonism in old age. J Nutr Health Aging 2018;22:1211–1215.ArticlePubMedPMCPDF
- 32. Tosukhowong P, Boonla C, Dissayabutra T, Kaewwilai L, Muensri S, Chotipanich C, et al. Biochemical and clinical effects of Whey protein supplementation in Parkinson’s disease: a pilot study. J Neurol Sci 2016;367:162–170.ArticlePubMed
- 33. Phillips MCL, Murtagh DKJ, Gilbertson LJ, Asztely FJS, Lynch CDP. Low-fat versus ketogenic diet in Parkinson’s disease: a pilot randomized controlled trial. Mov Disord 2018;33:1306–1314.ArticlePubMedPMC
- 34. Ludvigsson JF, Olsson T, Ekbom A, Montgomery SM. A population-based study of coeliac disease, neurodegenerative and neuroinflammatory diseases. Aliment Pharmacol Ther 2007;25:1317–1327.ArticlePubMed
- 35. Liu Y, Zhang BS. Serum 25-hydroxyvitamin D predicts severity in Parkinson’s disease patients. Neurol Sci 2014;35:67–71.ArticlePubMedPDF
- 36. Hiller AL, Murchison CF, Lobb BM, O’Connor S, O’Connor M, Quinn JF. A randomized, controlled pilot study of the effects of vitamin D supplementation on balance in Parkinson’s disease: does age matter? PLoS One 2018;13:e0203637.ArticlePubMedPMC
- 37. Suzuki M, Yoshioka M, Hashimoto M, Murakami M, Noya M, Takahashi D, et al. Randomized, double-blind, placebo-controlled trial of vitamin D supplementation in Parkinson disease. Am J Clin Nutr 2013;97:1004–1013.ArticlePubMedPDF
- 38. Taghizadeh M, Tamtaji OR, Dadgostar E, Daneshvar Kakhaki R, Bahmani F, Abolhassani J, et al. The effects of omega-3 fatty acids and vitamin E co-supplementation on clinical and metabolic status in patients with Parkinson’s disease: a randomized, double-blind, placebo-controlled trial. Neurochem Int 2017;108:183–189.ArticlePubMed
- 39. Tamtaji OR, Taghizadeh M, Aghadavod E, Mafi A, Dadgostar E, Daneshvar Kakhaki R, et al. The effects of omega-3 fatty acids and vitamin E cosupplementation on gene expression related to inflammation, insulin and lipid in patients with Parkinson’s disease: a randomized, double-blind, placebo-controlled trial. Clin Neurol Neurosurg 2019;176:116–121.ArticlePubMed
- 40. Liu D, Ke Z, Luo J. Thiamine deficiency and neurodegeneration: the interplay among oxidative stress, endoplasmic reticulum stress, and autophagy. Mol Neurobiol 2017;54:5440–5448.ArticlePubMedPDF
- 41. Coimbra CG, Junqueira VB. High doses of riboflavin and the elimination of dietary red meat promote the recovery of some motor functions in Parkinson’s disease patients. Braz J Med Biol Res 2003;36:1409–1417.ArticlePubMedPDF
- 42. Ford TC, Downey LA, Simpson T, McPhee G, Oliver C, Stough C. The effect of a high-dose vitamin B multivitamin supplement on the relationship between brain metabolism and blood biomarkers of oxidative stress: a randomized control trial. Nutrients 2018;10:1860.ArticlePubMedPMC
- 43. Ozer F, Meral H, Hanoglu L, Aydemir T, Yilsen M, Cetin S, et al. Plasma homocysteine levels in patients treated with levodopa: motor and cognitive associations. Neurol Res 2006;28:853–858.ArticlePubMed
- 44. Mischley LK, Allen J, Bradley R. Coenzyme Q10 deficiency in patients with Parkinson’s disease. J Neurol Sci 2012;318:72–75.ArticlePubMedPMC
- 45. Seet RC, Lim EC, Tan JJ, Quek AM, Chow AW, Chong WL, et al. Does high-dose coenzyme Q10 improve oxidative damage and clinical outcomes in Parkinson’s disease? Antioxid Redox Signal 2014;21:211–217.ArticlePubMed
- 46. Shults CW, Oakes D, Kieburtz K, Beal MF, Haas R, Plumb S, et al. Effects of coenzyme Q10 in early Parkinson disease: evidence of slowing of the functional decline. Arch Neurol 2002;59:1541–1550.ArticlePubMed
- 47. Müller T, Büttner T, Gholipour AF, Kuhn W. Coenzyme Q10 supplementation provides mild symptomatic benefit in patients with Parkinson’s disease. Neurosci Lett 2003;341:201–204.ArticlePubMed
- 48. Storch A, Jost WH, Vieregge P, Spiegel J, Greulich W, Durner J, et al. Randomized, double-blind, placebo-controlled trial on symptomatic effects of coenzyme Q(10) in Parkinson disease. Arch Neurol 2007;64:938–944.ArticlePubMed
- 49. Yoritaka A, Kawajiri S, Yamamoto Y, Nakahara T, Ando M, Hashimoto K, et al. Randomized, double-blind, placebo-controlled pilot trial of reduced coenzyme Q10 for Parkinson’s disease. Parkinsonism Relat Disord 2015;21:911–916.ArticlePubMed
- 50. Barichella M, Pacchetti C, Bolliri C, Cassani E, Iorio L, Pusani C, et al. Probiotics and prebiotic fiber for constipation associated with Parkinson disease: an RCT. Neurology 2016;87:1274–1280.ArticlePubMed
- 51. Borzabadi S, Oryan S, Eidi A, Aghadavod E, Daneshvar Kakhaki R, Tamtaji OR, et al. The effects of probiotic supplementation on gene expression related to inflammation, insulin and lipid in patients with Parkinson’s disease: a randomized, double-blind, placebo-controlled trial. Arch Iran Med 2018;21:289–295.PubMed
- 52. Chodzko-Zajko WJ, Proctor DN, Singh MAF, Minson CT, Nigg CR, Salem GR, et al. Exercise and physical activity for older adults. Medicine & Science in Sports & Exercise 2009;41:1510–1530.Article
- 53. Combs-Miller SA, Moore ES. Predictors of outcomes in exercisers with Parkinson disease: a two-year longitudinal cohort study. NeuroRehabilitation 2019;44:425–432.ArticlePubMed
- 54. da Silva FC, Iop RDR, de Oliveira LC, Boll AM, de Alvarenga JGS, Gutierres Filho PJB, et al. Effects of physical exercise programs on cognitive function in Parkinson’s disease patients: a systematic review of randomized controlled trials of the last 10 years. PLoS One 2018;13:e0193113.ArticlePubMedPMC
- 55. Santos D, Mahoney JR, Allali G, Verghese J. Physical activity in older adults with mild Parkinsonian signs: a cohort study. J Gerontol A Biol Sci Med Sci 2018;73:1682–1687.ArticlePubMedPDF
- 56. Coe S, Franssen M, Collett J, Boyle D, Meaney A, Chantry R, et al. Physical activity, fatigue, and sleep in people with Parkinson’s disease: a secondary per protocol analysis from an intervention trial. Parkinsons Dis 2018;2018:1517807.ArticlePubMedPMCPDF
- 57. Wu PL, Lee M, Huang TT. Effectiveness of physical activity on patients with depression and Parkinson’s disease: a systematic review. PLoS One 2017;12:e0181515.ArticlePubMedPMC
- 58. Rafferty MR, Prodoehl J, Robichaud JA, David FJ, Poon C, Goelz LC, et al. Effects of 2 years of exercise on gait impairment in people with Parkinson disease: the PRET-PD randomized trial. J Neurol Phys Ther 2017;41:21–30.ArticlePubMedPMC
- 59. Landers MR, Navalta JW, Murtishaw AS, Kinney JW, Pirio Richardson S. A high-intensity exercise boot camp for Persons with Parkinson disease: a phase II, pragmatic, randomized clinical trial of feasibility, safety, signal of efficacy, and disease mechanisms. J Neurol Phys Ther 2019;43:12–25.ArticlePubMed
- 60. Zoladz JA, Majerczak J, Zeligowska E, Mencel J, Jaskolski A, Jaskolska A, et al. Moderate-intensity interval training increases serum brain-derived neurotrophic factor level and decreases inflammation in Parkinson’s disease patients. J Physiol Pharmacol 2014;65:441–448.PubMed
- 61. Corcos DM, Robichaud JA, David FJ, Leurgans SE, Vaillancourt DE, Poon C, et al. A two-year randomized controlled trial of progressive resistance exercise for Parkinson’s disease. Mov Disord 2013;28:1230–1240.ArticlePubMedPMC
- 62. Cheung C, Bhimani R, Wyman JF, Konczak J, Zhang L, Mishra U, et al. Effects of yoga on oxidative stress, motor function, and non-motor symptoms in Parkinson’s disease: a pilot randomized controlled trial. Pilot Feasibility Stud 2018;4:162.ArticlePubMedPMCPDF
- 63. Ni M, Signorile JF, Mooney K, Balachandran A, Potiaumpai M, Luca C, et al. Comparative effect of power training and high-speed yoga on motor function in older patients with Parkinson disease. Arch Phys Med Rehabil 2016;97:345–354.e15.ArticlePubMed
- 64. Hawkins BL, Van Puymbroeck M, Walter A, Sharp J, Woshkolup K, Urrea-Mendoza E, et al. Perceived activities and participation outcomes of a yoga intervention for individuals with Parkinson’s disease: a mixed methods study. Int J Yoga Therap 2018;28:51–61.ArticlePubMedPDF
- 65. Amano S, Nocera JR, Vallabhajosula S, Juncos JL, Gregor RJ, Waddell DE, et al. The effect of Tai Chi exercise on gait initiation and gait performance in persons with Parkinson’s disease. Parkinsonism Relat Disord 2013;19:955–960.ArticlePubMed
- 66. Li F, Harmer P, Liu Y, Eckstrom E, Fitzgerald K, Stock R, et al. A randomized controlled trial of patient-reported outcomes with tai chi exercise in Parkinson’s disease. Mov Disord 2014;29:539–545.ArticlePubMed
- 67. Song R, Grabowska W, Park M, Osypiuk K, Vergara-Diaz GP, Bonato P, et al. The impact of Tai Chi and Qigong mind-body exercises on motor and non-motor function and quality of life in Parkinson’s disease: a systematic review and meta-analysis. Parkinsonism Relat Disord 2017;41:3–13.ArticlePubMedPMC
- 68. Hackney ME, Earhart GM. Tai Chi improves balance and mobility in people with Parkinson disease. Gait Posture 2008;28:456–460.ArticlePubMedPMC
- 69. Walker MP, Brakefield T, Morgan A, Hobson JA, Stickgold R. Practice with sleep makes perfect: sleep-dependent motor skill learning. Neuron 2002;35:205–211.ArticlePubMed
- 70. Rui Z, Qingling C, Xinyue Z, Xin Z, Weihong L. The related factors of sleep benefit in Parkinson’s disease: a systematic review and meta-analysis. PLoS One 2019;14:e0212951.ArticlePubMedPMC
- 71. Kwok JYY, Kwan JCY, Auyeung M, Mok VCT, Chan HYL. The effects of yoga versus stretching and resistance training exercises on psychological distress for people with mild-to-moderate Parkinson’s disease: study prxotocol for a randomized controlled trial. Trials 2017;18:509.ArticlePubMedPMCPDF
- 72. Gao X, Cassidy A, Schwarzschild MA, Rimm EB, Ascherio A. Habitual intake of dietary flavonoids and risk of Parkinson disease. Neurology 2012;78:1138–1145.ArticlePubMedPMC
- 73. Sang Q, Liu X, Wang L, Qi L, Sun W, Wang W, et al. Curcumin protects an SH-SY5Y cell model of Parkinson’s disease against toxic injury by regulating HSP90. Cell Physiol Biochem 2018;51:681–691.ArticlePubMed
- 74. Wang XS, Zhang ZR, Zang MM, Sun MX, Wang WW, Xie CL. Neuroprotective properties of curcumin in toxin-based animal models of Parkinson’s disease: a systematic experiment literatures review. BMC Complement Altern Med 2017;17:412.ArticlePubMedPMCPDF
- 75. Hadjivassiliou M, Rao DG, Grìnewald RA, Aeschlimann DP, Sarrigiannis PG, Hoggard N, et al. Neurological dysfunction in coeliac disease and non-coeliac gluten sensitivity. Am J Gastroenterol 2016;111:561–567.ArticlePubMedPMCPDF
- 76. Vinagre-Aragón A, Zis P, Grunewald RA, Hadjivassiliou M. Movement disorders related to gluten sensitivity: a systematic review. Nutrients 2018;10:1034.ArticlePubMedPMC
- 77. Fujita S, Volpi E. Amino acids and muscle loss with aging. J Nutr 2006;136(1 Suppl):277S–280S.ArticlePubMedPMCPDF
- 78. Kieffer DA, Martin RJ, Adams SH. Impact of dietary fibers on nutrient management and detoxification organs: gut, liver, and kidneys. Adv Nutr 2016;7:1111–1121.ArticlePubMedPMC
- 79. Lebouvier T, Neunlist M, Bruley des Varannes S, Coron E, Drouard A, N’Guyen JM, et al. Colonic biopsies to assess the neuropathology of Parkinson’s disease and its relationship with symptoms. PLoS One 2010;5:e12728.ArticlePubMedPMC
- 80. Leech B, McIntyre E, Steel A, Sibbritt D. Risk factors associated with intestinal permeability in an adult population: A systematic review. Int J Clin Pract 2019;73:e13385.ArticlePubMed
- 81. Gerhardt S, Mohajeri MH. Changes of colonic bacterial composition in Parkinson’s disease and other neurodegenerative diseases. Nutrients 2018;10:708.ArticlePubMedPMC
- 82. Hill-Burns EM, Debelius JW, Morton JT, Wissemann WT, Lewis MR, Wallen ZD, et al. Parkinson’s disease and Parkinson’s disease medications have distinct signatures of the gut microbiome. Mov Disord 2017;32:739–749.ArticlePubMedPMC
- 83. Jeejeebhoy K. Malnutrition, fatigue, frailty, vulnerability, sarcopenia and cachexia: overlap of clinical features. Curr Opin Clin Nutr Metab Care 2012;15:213–219.ArticlePubMed
- 84. Kalyani HHN, Sullivan K, Moyle G, Brauer S, Jeffrey ER, Roeder L, et al. Effects of dance on gait, cognition, and dual-tasking in Parkinson’s disease: a systematic review and meta-analysis. J Parkinsons Dis 2019;9:335–349.ArticlePubMed
- 85. Ćwiękała-Lewis KJ, Gallek M, Taylor-Piliae RE. The effects of Tai Chi on physical function and well-being among persons with Parkinson’s disease: a systematic review. J Bodyw Mov Ther 2017;21:414–421.ArticlePubMed
- 86. Silva-Batista C, de Brito LC, Corcos DM, Roschel H, de Mello MT, Piemonte MEP, et al. Resistance training improves sleep quality in subjects with moderate Parkinson’s disease. J Strength Cond Res 2017;31:2270–2277.ArticlePubMed
- 87. Besedovsky L, Lange T, Haack M. The sleep-immune crosstalk in health and disease. Physiol Rev 2019;99:1325–1380.ArticlePubMedPMC
- 88. Russell AL, Tasker JG, Lucion AB, Fiedler J, Munhoz CD, Wu TJ, et al. Factors promoting vulnerability to dysregulated stress reactivity and stress-related disease. J Neuroendocrinol 2018;30:e12641.ArticlePubMedPMC
- 89. Ide K, Yamada H, Umegaki K, Mizuno K, Kawakami N, Hagiwara Y, et al. Lymphocyte vitamin C levels as potential biomarker for progression of Parkinson’s disease. Nutrition 2015;31:406–408.ArticlePubMed
- 90. Jenner P, Olanow CW. Oxidative stress and the pathogenesis of Parkinson’s disease. Neurology 1996;47(6 Suppl 3):S161–S170.ArticlePubMed
- 91. Hodges RE, Minich DM. Modulation of metabolic detoxification pathways using foods and food-derived components: a scientific review with clinical application. J Nutr Metab 2015;2015:760689.ArticlePubMedPMCPDF
- 92. Monti DA, Zabrecky G, Kremens D, Liang TW, Wintering NA, Cai J, et al. N-acetyl cysteine may support dopamine neurons in Parkinson’s disease: preliminary clinical and cell line data. PLoS One 2016;11:e0157602.ArticlePubMedPMC
- 93. Suzuki M, Yoshioka M, Hashimoto M, Murakami M, Noya M, Takahashi D, et al. Randomized, double-blind, placebo-controlled trial of vitamin D supplementation in Parkinson disease. Am J Clin Nutr 2013;97:1004–1013.ArticlePubMedPDF
- 94. Scott D, Ebeling PR. Vitamin D and public health. Int J Environ Res Public Health 2019;16:848.ArticlePubMedPMC
- 95. Heaney RP, Dowell MS, Hale CA, Bendich A. Calcium absorption varies within the reference range for serum 25-hydroxyvitamin D. J Am Coll Nutr 2003;22:142–146.ArticlePubMed
- 96. Costantini A, Pala MI, Grossi E, Mondonico S, Cardelli LE, Jenner C, et al. Long-term treatment with high-dose thiamine in Parkinson disease: an open-label pilot study. J Altern Complement Med 2015;21:740–747.ArticlePubMed
- 97. Warren Olanow C, Obeso JA. Levodopa toxicity and Parkinson disease: still a need for equipoise. Neurology 2011;77:1416–1417.ArticlePubMed
- 98. Radler DR, Lister T. Nutrient deficiencies associated with nutrition-focused physical findings of the oral cavity. Nutr Clin Pract 2013;28:710–721.ArticlePubMed
- 99. Hooper L, Ashton K, Harvey LJ, Decsi T, Fairweather-Tait SJ. Assessing potential biomarkers of micronutrient status by using a systematic review methodology: methods. Am J Clin Nutr 2009;89:1953S–1959S.ArticlePubMedPDF
- 100. National Institutes of Health Office of Dietary Supplements. Omega-3 fatty acids. [cited 2019 Nov 9]. Available from: https://ods.od.nih.gov/factsheets/Omega3FattyAcids-HealthProfessional/.
REFERENCES
Figure & Data
References
Citations
Citations to this article as recorded by 
- Vitamin D supplementation in later life: a systematic review of efficacy and safety in movement disorders
Carl N. Homann, Barbara Homann, Gerd Ivanic, Tadea Urbanic-Purkart
Frontiers in Aging Neuroscience.2024;[Epub] CrossRef - U.S. Tax Credits to Promote Practical Proactive Preventative Care for Parkinson’s Disease
Michael S. Okun
Journal of Parkinson's Disease.2024; 14(2): 221. CrossRef - A Qualitative Analysis of Experiences With Food-Related Activities Among People Living With Parkinson Disease and Their Care-Partners
Christine C. Ferguson, Seung Eun Jung, Jeannine C. Lawrence, Joy W. Douglas, Anne Halli-Tierney, Chuong Bui, Amy C. Ellis
Journal of Applied Gerontology.2023; 42(1): 131. CrossRef - Mobile health technology, exercise adherence and optimal nutrition post rehabilitation among people with Parkinson’s Disease (mHEXANUT) – a randomized controlled trial protocol
Sigrid Ryeng Alnes, Ellisiv Lærum-Onsager, Asta Bye, Annette Vistven, Erika Franzén, Mette Holst, Therese Brovold
BMC Neurology.2023;[Epub] CrossRef - Association between smoking and all-cause mortality in Parkinson’s disease
Seo Yeon Yoon, You Hyun Park, Sang Chul Lee, Jee Hyun Suh, Seung Nam Yang, Dae Ryong Kang, Yong Wook Kim
npj Parkinson's Disease.2023;[Epub] CrossRef - Molecular insights into the pathogenic impact of vitamin D deficiency in neurological disorders
Md Jamir Anwar, Sattam Khulaif Alenezi, Ahmad Hamad Alhowail
Biomedicine & Pharmacotherapy.2023; 162: 114718. CrossRef - Role of Nutraceuticals and Physical Activity in Parkinson's Disease Risk
and Lifestyle Management
Pranay Wal, Himangi Vig, Ankita Wal, Shruti Rathore, Shiv Shanker Pandey, Nem Kumar Jain, Ashish Srivastava
Current Aging Science.2023; 16(3): 170. CrossRef - Social Control and Health Behaviors Among Individuals Living with Parkinson’s Disease: A Pilot Study
Shahrzad Mavandadi, Alejandro Interian, Steven Sayers, Roseanne Dobkin, Daniel Weintraub
International Journal of Behavioral Medicine.2023;[Epub] CrossRef - Gut microbiome-based dietary intervention in Parkinson disease subject: A case report
Ayesha Sulthana, Shasthara Paneyala, Sindhu H.S., Meghana Kowlagi Narayan, Tousif Ahmed Hediyal, Sonali Sharma, Arunsaikiran Senthilkumar, Paul Dave, Arehally M. Mahalakshmi, Saravana Babu Chidambaram, Tanya M. Monaghan, Dinanath Sulakhe
International Journal of Nutrition, Pharmacology, Neurological Diseases.2023; 13(3): 158. CrossRef - Effect of vitamin D and other indicators of phosphorus-calcium metabolism on cognitive functions and quality of life in patients with Parkinson's disease
D. A. Novotnyy, N. G. Zhukova, L. P. Shperling, V. A. Stolyarova, I. A. Zhukova, A. E. Agasheva, S. V. Shtaimets, O. A. Druzhinina, I. V. Shirokikh
Neurology, Neuropsychiatry, Psychosomatics.2022; 14(1): 38. CrossRef - Do Naturally Occurring Antioxidants Protect Against Neurodegeneration
of the Dopaminergic System? A Systematic Revision in Animal Models of
Parkinson's Disease
Carmen Costas, Lilian R.F. Faro
Current Neuropharmacology.2022; 20(2): 432. CrossRef - Laboratory prognostic factors for the long-term survival of multiple system atrophy
Jung Hwan Shin, Han-Joon Kim, Chan Young Lee, Hee Jin Chang, Kyung Ah Woo, Beomseok Jeon
npj Parkinson's Disease.2022;[Epub] CrossRef - Association Between Smoking and All-Cause Mortality in Parkinson's Disease
Seo Yeon Yoon, You Hyun Park, Sang Chul Lee, Jee Hyun Suh, Seung Nam Yang, Dae Ryong Kang, Yong Wook Kim
SSRN Electronic Journal .2022;[Epub] CrossRef
Comments on this article
 PubReader
PubReader ePub Link
ePub Link Cite
Cite
